 E-submission
E-submission
Articles
- Page Path
- HOME > J Liver Cancer > Volume 21(2); 2021 > Article
-
Review Article
Liver transplantation for hepatocellular carcinoma with portal vein tumor thrombosis -
Sang Jin Kim1,2
 , Jong Man Kim3
, Jong Man Kim3 -
Journal of Liver Cancer 2021;21(2):105-112.
DOI: https://doi.org/10.17998/jlc.2021.03.17
Published online: September 2, 2021
1Division of Hepatobiliopancreas and Transplant Surgery, Korea University Ansan Hospital, Ansan, Korea
2Department of Surgery, Korea University College of Medicine, Seoul, Korea
3Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
-
Corresponding author: Jong Man Kim, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea,
Tel. +82-2-3410-1719, Fax. +82-2-3410-0040, E-mail: yjongman21@gmail.com
Copyright © 2021 by The Korean Liver Cancer Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 5,000 Views
- 221 Downloads
- 3 Citations
Abstract
- Traditionally, liver transplantation for hepatocellular carcinoma with portal vein tumor thrombosis is not recommended. However, with recent developments in locoregional therapies for hepatocellular carcinoma, more aggressive treatments have been attempted for advanced hepatocellular carcinoma. Recently, various studies on locoregional therapies for downstaging followed by living donor liver transplantation reported inspiring overall survival and recurrence-free survival of patients. These downstaging procedures included three-dimensional conformal radiation therapy, trans-arterial chemoembolization, stereotactic body radiation therapy, trans-arterial radioembolization, hepatic arterial infusion chemotherapy and combinations of these therapies. Selection of the optimal downstaging protocol should depend on tumor location, biology and background liver status. The risk factors affecting outcome include pre-downstaging alpha-fetoprotein values, delta alpha-fetoprotein values, disappearance of portal vein tumor thrombosis on imaging and meeting the Milan criteria or not after downstaging. For hepatocellular carcinoma with portal vein tumor thrombosis, downstaging procedure with liver transplantation in mind would be helpful. If the reaction of the downstaged tumor is good, liver transplantation may be performed.
- Liver transplantation (LT) is an effective treatment for nonresectable hepatocellular carcinoma (HCC) with liver cirrhosis. However, LT requires adequate conditions to be successful, including tumor size, tumor number, vascular invasion, and extrahepatic metastasis. The Milan criteria (1996) and University of California San Francisco criteria (UCSF, 2001) have been generally used for selection; while these two criteria conflict regarding ideal tumor size, they agree that the absence of vascular invasion is an indication for LT.1,2 Vascular invasion is a poor prognostic factor for HCC, resulting in a median survival time of two to 12 months, and is regarded as a contraindication for LT.3 Sorafenib is the only recommended treatment for advanced HCC according to the Barcelona Clinic Liver Cancer (BCLC) staging system. However, the outcome of sorafenib-alone treatment is still poor, while advanced HCC is relatively common with a 10% to 40% prevalence rate in total HCC population.4,5 Thus, medical centers are expanding their treatment profile for advanced HCC, many of which have been well-reviewed in a recent article.6 As locoregional therapy develops and good outcomes are achieved with advanced HCC, an increasing variety of downstaging procedures for advanced HCC followed by LT are being performed. We seek herein to review living donor LT (LDLT) outcomes after downstaging for HCC with portal vein tumor thrombosis (PVTT).
INTRODUCTION
- Ultrasound (US), contrast-enhanced US (CEUS), computed tomography (CT), and magnetic resonance imaging (MRI) are generally used as diagnostic methods for HCC with PVTT. CEUS is a cheap and highly sensitive method for differential diagnosis of malignant PVTT and benign lesions. 7 Malignant PVTT shows increased enhancement in the arterial phase and rapid wash-out in the portal/delayed phase, similar to HCC.8 CT imaging and MRI are usually used for diagnosing liver status or collateral vessels and for HCC evaluation and may also be useful for differentiating benign lesions and malignant PVTT with a sensitivity and specificity of around 90%.9,10 18-fluorodeoxyglucose positron emission tomography (PET) can reveal the metabolic activity of malignant PVTT. One study showed that PET/CT can differentiate between benign lesions and malignant PVTT with a sensitivity of 93.6% and a specificity of 80% when the criterion of maximum standardized uptake value (SUVmax) was set to more than 3.35.11
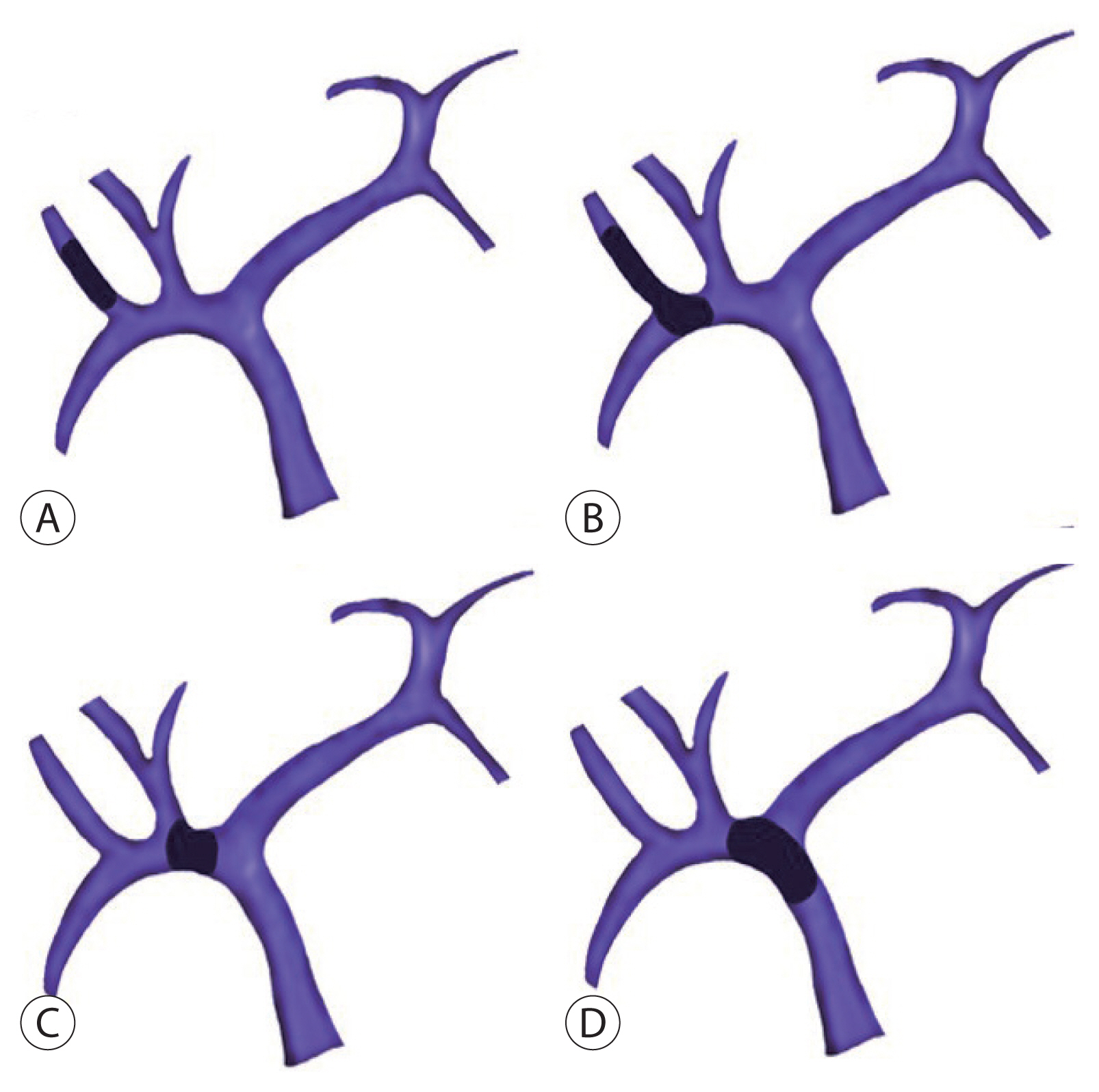
- There are some studies that have classified the grade of PVTT in many ways. One of the well-known classifications is from the Liver Cancer Study Group of Japan.12 Under this scheme, a PVTT case is distinguished as one of the following four grades: Vp1, tumor thrombus distal to the second-order branch of the portal vein but not in the second-order branch; Vp2, tumor invasion of the second-order branch; Vp3, tumor invasion of the first-order branch; and Vp4, tumor invasion of the main portal vein (MPV) and/or the portal vein branch contralateral to the primarily involved lobe (Fig. 1).
HCC WITH PVTT DIAGNOSIS AND STAGING
- Sorafenib, a multi-targeting tyrosine kinase inhibitor, is recommended for the treatment for HCC with PVTT according to BCLC staging.13 This drug supported relatively longer survival rates relative to the placebo in two phase III trials.14,15 Also, the combination of sorafenib and locoregional therapies has been trialed; here, sorafenib combined with transarterial chemoembolization (TACE) or sorafenib combined with radiofrequency ablation (RFA) for HCC with PVTT led to relatively better outcomes than sorafenib-alone treatment.16,17 However, these combination therapies possess a risk for high adverse events such as abdominal pain, hand-foot skin reactions, asthenia, diarrhea, and weight loss.
- TACE, which has been accepted as palliative therapy for multinodular HCC in a still-functioning liver, has a risk for inducing ischemia of the normal liver when insufficient collateral vessels exist around a tumor-obstructed portal vein.6,18 However, in selective cases, TACE achieved better outcomes than those of the supportive group in the setting of HCC with PVTT. A recent study reviewed 1,933 patients who received TACE for HCC with PVTT and reported one-, three-, and five-year overall survival (OS) rates of 29%, 4%, and 1%, respectively.19 Sorafenib, which expresses anti-angiogenic activity—which may suppress the angiogenic factor released due to hypoxia after TACE—can be combined with TACE, resulting in better OS rates.20 There is also a recently inspiring result of combined TACE and sorafenib with a three-year OS of 86.1% in a phase II trial study.21
- Steady efforts to explore the impact of radiation therapy (RT) on HCC with PVTT revealed some effects even despite the risk of radiation-induced liver disease (RILD). However, one study reported that a high dose of radiation applied to a large liver volume (V30Gy >28.1%) may cause RILD, resulting in jaundice, hepatomegaly, ascites, and an elevated Child-Pugh score.22 To avoid injury to nontumorous areas of the liver, three-dimensional conformal RT (3D-CRT) was developed, which applies radiation highly selectively to the tumor and PVTT by modifying the radiation beam to match the shape of the tumor.23 Also, the use of a “dose-volume histogram” may guide radiation concentrated on the tumor.24 A recent propensity score-matching study showed that RT resulted in impressively longer median survival times as compared with sorafenib treatment in 56 of Vp3 or Vp4 PVTT patients (10.9 months vs. 4.8 months).25 Other investigations of stereotactic body RT (SBRT), proton beam therapy, and gamma knife radiosurgery showed comparable outcomes in HCC with PVTT.26,27
- Although there is a risk of complications such as vascular or biliary stricture due to mechanical and thermal injury, RFA has shown some effect on HCC with PVTT.28 Giorgio et al.29,30 introduced a technique in 2014 named “percutaneous RF thrombectomy,” which encompasses both HCC single nodules (3–5 cm) and intraportal tumoral extensions, reporting one-, three-, and five-year OS rates of 63%, 30% and 23% in 35 patients with HCC involving MPV tumor thrombus (Vp4). Conversely, the one-year survival rate in the control group (n=22 patients without any treatment) was 0% (P <0.0001), while the HCC necrosis and recanalization rate of the RFA group was 74%. Also, combined RFA and sorafenib achieved a significantly increased three-year survival rate (26%) in 49 patients as compared with that of sorafenib-alone treatment (0%) in 50 patients for HCC with Vp4 PVTT in a Western randomized control trial.17
- Transarterial radioembolization (TARE) reduces the risk of hepatic parenchymal ischemia as compared to TACE by delivering iodine-131-labeled lipiodol, iodine, or yttrium-90 selectively through the hepatic arteries supplying tumor.31 Adverse effects such as fever, nausea, and abdominal pain are usually manageable by conservative support. In some retrospective studies, TARE showed better survival outcomes than sorafenib-alone treatment.32,33 Although two recent phase III randomized controlled trials did not confirm the superiority of TARE than sorafenib, several TARE treatments have been studied to increase the therapeutic effect on HCC with PVTT.34,35
- Traditionally, systemic chemotherapy has not been used widely because its antitumor effect is weaker and it boasts high liver toxicity, especially in patients with liver cirrhosis. However, a recent study showed a method of infusing 5-fluorouracil (5-FU) and cisplatin into the hepatic arteries selectively in patients with advanced HCC, resulting in higher response rates and less adverse effects.36 This hepatic arterial infusion chemotherapy (HAIC) approach was relatively more effective than sorafenib-alone treatment in HCC with Vp2–4 PVTT.37
NONSURGICAL THERAPEUTIC OPTIONS FOR HCC WITH PVTT
- Although the recommended treatment for HCC with PVTT in BCLC classification is sorafenib, some studies have shown the better OS for surgical operation as compared with sorafenib therapy. This aggressive treatment must be individualized to the patient’s risk and tumor types.38 Depending on the location of PVTT and operator’s preference, three surgical treatments are usually adopted: hepatectomy for tumors with ipsilateral PVTT, en-bloc resection followed by portal vein reconstruction for tumors with PVTT extending beyond portal vein bifurcation, and thrombectomy for tumors with PVTT extending beyond portal vein bifurcation.39 These treatments demonstrated median OS rates of 0.91, 9.4, and 8.58 months (P =0.962), respectively, in one study with 88 patients. Another study with 113 patients with propensity score-matching reported significantly better OS in the enblock resection-treated group than in the thrombectomy–treated group (odds ratio, 1.471; P =0.017).40 Surgical resection is sometimes combined with other treatments such as adjuvant TACE, neoadjuvant RT, TARE, or concurrent chemoradiation therapy (CCRT) to prevent thrombus dissemination, lower the recurrence rate, and enhance the chance of survival.41–44 In the context of a downstaging procedure followed by surgery, the non-response of the alpha-feto protein (AFP) level seems to be a risk factor for tumor recurrence.
SURGICAL RESECTION OF HCC WITH PVTT
- LT has been also not recommended due to the high recurrence rate of HCC with PVTT, similarly to surgical resection in traditional guidelines. Furthermore, LT carries the ethical consideration of applying liver grafts to the most appropriate recipients due to the shortage of liver donors. However, LT medical technology is gradually improving for patients with HCC and many centers are attempting LDLT for advanced HCC nowadays. LDLT may lower the burden of graft shortage relative to deceased donor LT.
- Lee et al.45 studied 11 patients with advanced HCC who underwent LT at Seoul National University Hospital in South Korea and reported relatively good one-, three-, and five-year recurrence-free survival (RFS) rates of 63.9%, 45.5%, and 45.5% and one-, three-, and five-year OS rates of 72.7%, 63.6%, and 63.6%, respectively. Seven patients had Vp2 or 3 PVTT and four patients had Vp4 PVTT. Four patients received TACE after developing PVTT before transplantation. This study revealed some risk factors for patient death and recurrence, including MPV invasion, high AFP × ‘protein induced by the vitamin K absence/antagonist II’ (AP) score (≥20,000), high SUV ratio (tumor vs. background liver) in PET/CT (≥2.1), largest tumor size of more than 7 cm (univariate analysis due to the small case number). Among these factors, the high SUV ratio only affected the recurrence rate. Patients with low AP scores (<20,000, n=5 patients) did not experience tumor recurrence.
- With increasing outcomes of various locoregional therapies on HCC with PVTT, additional studies are more focused on LT after downstaging for HCC with PVTT. A recent study of 17 patients at Asan Medical Center, South Korea with HCC and major vascular invasion received downstaging by 3D-CRT and TACE followed by LT.46 Included patients were those in which HCC had invaded the right, left portal veins or MPV; or right, middle, or left hepatic vein. Two to three weeks after TACE (2–10 mL of Lipiodol [Guerbet LLC, Princeton, NJ, USA] and 1mg/kg of cisplatin with Gelfoam [Pfizer, New York, NY, USA]), RT was performed. The planned target margin of RT was 1 to 2 cm and the total radiation dose was decided while considering liver function, residual liver volume, and adjacent organ location. Following one month of downstaging, diagnostic imaging and checking tumor markers were conducted to confirm the treatment response, and then LT was performed. Six patients received LT subsequently, while 11 patients received additional locoregional therapy, resulting in a median interval between RT and LT of 5.1 months. With a rate of 82.4% for tumor thrombus complete response, 10 among 17 patients met Milan’s criteria just before LT. One- and three-year RFS rates were 70.6% and 57.8% and one- and three-year OS rates were 87.4% and 60.5%, respectively. Notably, the three-year disease-free survival and OS rates of patients who met the Milan criteria just before LT were significantly better than those without Milan criteria (disease-free survival rate: 88.9% vs. 14.3%, P =0.007; OS rate: 80% vs. 25.7%, P =0.010). Meanwhile, another study covered five patients with HCC and Vp1–3 PVTT who received LT after downstaging involving 3D-CRT after TACE47 at Samsung Medical Center, South Korea. Here, the interval between TACE and 3D-CRT was usually two weeks (one patient did not receive TACE) and the median RFS and OS lengths were 11.7 and 35.2 months, respectively. This study also compared the outcomes between patient who received LT after downstaging and 10 patients who received RT-alone without LT by propensity score-matching, revealing significant differences in median OS times (32.5 vs. 12.2 months; P <0.01).
- SBRT, which administers high-dose radiation using several beams from different angles focused on the tumor, has also been attempted for the downstaging of advanced HCC before LDLT in a recent study.48 Downstaging (SBRT with/or without TARE, TACE, or RFA) for patients with Vp3 and 4 PVTT was performed when patient’s serum bilirubin level was lower than 5 mg/dL without ascites and the nontumoral liver volume was greater than 700 mL. Study participants were re-evaluated after four to six weeks and received LDLT if there was no PVTT. For Vp1 and 2 PVTT patients, LDLT was performed 10 to 15 days after SBRT on tumor thrombus. Among 43 patients, 27 (63%) patients showed no tumor thrombus after SBRT and, finally, 25 patients received LDLT. This study compared the three groups of patients with PVTT who received LDLT after downstaging (DS group, n=25), patients with PVTT who received only LDLT without downstaging (non-DS group, n=21), and patients without PVTT who received only LDLT (upfront LT group, n=405), respectively. The DS group showed one-, three-, and five-year OS rates of 75%, 53%, and 53% and RFS rates of 78%, 78%, and 52%, respectively. Also, after censoring the two postoperative death cases which died within two months after LT, the five-year OS (57% vs. 48%) and RFS (51% vs. 40%) rates of the DS group (n=23) were slightly higher than those of the non-DS group (n=20), albeit without significant differences between them. Moreover, the five-year OS (57% vs. 65%) and RFS (51% vs. 66%) rates of the DS group were slightly lower than those of the upfront LT group after censoring postoperative death, again without significant differences. In the DS group, tumor grade III/IV was a risk factor for reduced OS, while high preoperative AFP (>400 ng/mL) and low delta AFP (AFP change between before and after downstaging, <2,000 ng/mL) were poor prognostic factors for RFS. Meanwhile, there are other studies of downstaging prior to LT showing acceptable outcomes;49,50 one study noted that the median RFS time of four patients who received TARE as downstaging was 39 months.51
- CCRT was also attempted as a downstaging method of HCC with PVTT before LDLT.52 In one study, RT combined with 5-FU was administered during five weeks and additional HAIC (5-FU/cisplatin combination) was introduced for about three to 12 months in four-week intervals at Severance Hospital, South Korea. All eight patients achieved successful downstaging, with no PVTT, and received LDLT. The one-year OS rate was 87.5% and the median survival time was 33 months.
- Immunotherapy is not yet widely used for downstaging method of HCC with PVTT before LT. However, there is a case report of using nivolumab, an immune checkpoint inhibitor before LT in a patient with HCC outside Milan criteria (due to 4 lesions in liver) resulting patient surviving more than one-year without tumor recurrence.53 This result showed the potential for the role of immunotherapy in downstaging method of HCC with PVTT. In this setting, immune therapy just prior to or after LT may be fatal due to 4-week half-life and hepatotoxicity of nivolumab.54
LIVER TRANSPLANTATION WITH OR WITHOUT DOWNSTAGING FOR HCC WITH PVTT
- To this day, the American Association for the Study of Liver Disease and European Association for the Study of the Liver guidelines do not offer suggestions for LT after downstaging for HCC with PVTT.55,56 However, given that more recent studies of downstaging procedures have promoted favorable outcomes, LT after downstaging is increasingly worth considering for HCC with PVTT. Although these trials are not of excellent quality, this approach still shows better outcomes than sorafenib-alone treatment. Due to the small number of existing studies, more trials and evidence are needed before stronger conclusions can be drawn.
- There are a few common things that should be considered. First, the optimal downstaging protocol is important to the outcome. RT, TACE, or TARE can be considered according to patients and tumor status. Second, risk factors affecting OS and RFS rates should be considered. The predownstaging AFP value, delta AFP value, disappearance of PVTT on imaging, and meeting the Milan criteria or not after downstaging may be considered.
- Therefore, for HCC with PVTT, locoregional therapy with LT in mind would be helpful. After that, if the reaction of the downstaged tumor is good, then LT may be performed in selected cases; otherwise, other therapies can be considered.
CONCLUSION
-
Conflicts of Interest
The authors declare no conflict of interest.
-
Ethics Statement
This review article is fully based on the articles which was already published and did not involve additional patient participants. Therefore, IRB approval is not necessary.
-
Funding Statement
No funding to declare.
-
Data Availability
Data sharing not applicable to this article as no datasets were generated or analyzed during the study.
-
Author Contribution
Conception and design, data acquisition, drafting the article: SJK.
Conception and design, critical revision of the article: JMK.
All authors have reviewed and approved the final version of manuscript.
Article information
- 1. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996;334:693−699.ArticlePubMed
- 2. Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook A, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology 2001;33:1394−1403.ArticlePubMed
- 3. Minagawa M, Makuuchi M. Treatment of hepatocellular carcinoma accompanied by portal vein tumor thrombus. World J Gastroenterol 2006;12:7561−7567.ArticlePubMedPMC
- 4. Lee YH, Hsu CY, Huang YH, Hsia CY, Chiou YY, Su CW, et al. Vascular invasion in hepatocellular carcinoma: prevalence, determinants and prognostic impact. J Clin Gastroenterol 2014;48:734−741.PubMed
- 5. Shen J, Wen J, Li C, Wen T, Yan L, Li B, et al. The prognostic value of microvascular invasion in early-intermediate stage hepatocelluar carcinoma: a propensity score matching analysis. BMC Cancer 2018;18:278. ArticlePubMedPMC
- 6. Cerrito L, Annicchiarico BE, Iezzi R, Gasbarrini A, Pompili M, Ponziani FR. Treatment of hepatocellular carcinoma in patients with portal vein tumor thrombosis: beyond the known frontiers. World J Gastroenterol 2019;25:4360−4382.ArticlePubMedPMC
- 7. Tarantino L, Francica G, Sordelli I, Esposito F, Giorgio A, Sorrentino P, et al. Diagnosis of benign and malignant portal vein thrombosis in cirrhotic patients with hepatocellular carcinoma: color Doppler US, contrast-enhanced US, and fine-needle biopsy. Abdom Imaging 2006;31:537−544.ArticlePubMed
- 8. Rossi S, Rosa L, Ravetta V, Cascina A, Quaretti P, Azzaretti A, et al. Contrast-enhanced versus conventional and color Doppler sonography for the detection of thrombosis of the portal and hepatic venous systems. AJR Am J Roentgenol 2006;186:763−773.ArticlePubMed
- 9. Tublin ME, Dodd GD 3rd, Baron RL. Benign and malignant portal vein thrombosis: differentiation by CT characteristics. AJR Am J Roentgenol 1997;168:719−723.ArticlePubMed
- 10. Sandrasegaran K, Tahir B, Nutakki K, Akisik FM, Bodanapally U, Tann M, et al. Usefulness of conventional MRI sequences and diffusion-weighted imaging in differentiating malignant from benign portal vein thrombus in cirrhotic patients. AJR Am J Roentgenol 2013;201:1211−1219.ArticlePubMed
- 11. Hu S, Zhang J, Cheng C, Liu Q, Sun G, Zuo C. The role of 18F-FDG PET/CT in differentiating malignant from benign portal vein thrombosis. Abdom Imaging 2014;39:1221−1227.ArticlePubMed
- 12. Ikai I, Arii S, Okazaki M, Okita K, Omata M, Kojiro M, et al. Report of the 17th nationwide follow-up survey of primary liver cancer in Japan. Hepatol Res 2007;37:676−691.ArticlePubMed
- 13. Forner A, Reig ME, de Lope CR, Bruix J. Current strategy for staging and treatment: the BCLC update and future prospects. Semin Liver Dis 2010;30:61−74.ArticlePubMed
- 14. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008;359:378−390.ArticlePubMed
- 15. Cheng AL, Guan Z, Chen Z, Tsao CJ, Qin S, Kim JS, et al. Efficacy and safety of sorafenib in patients with advanced hepatocellular carcinoma according to baseline status: subset analyses of the phase III Sorafenib Asia-Pacific trial. Eur J Cancer 2012;48:1452−1465.ArticlePubMed
- 16. Park JW, Kim YJ, Kim DY, Bae SH, Paik SW, Lee YJ, et al. Sorafenib with or without concurrent transarterial chemoembolization in patients with advanced hepatocellular carcinoma: the phase III STAH trial. J Hepatol 2019;70:684−691.ArticlePubMed
- 17. Giorgio A, Merola MG, Montesarchio L, Merola F, Santoro B, Coppola C, et al. Sorafenib combined with radio-frequency ablation compared with sorafenib alone in treatment of hepatocellular carcinoma invading portal vein: a western randomized controlled trial. Anticancer Res 2016;36:6179−6183.ArticlePubMed
- 18. Yin J, Bo WT, Sun J, Xiang X, Lang JY, Zhong JH, et al. New evidence and perspectives on the management of hepatocellular carcinoma with portal vein tumor thrombus. J Clin Transl Hepatol 2017;5:169−176.PubMedPMC
- 19. Silva JP, Berger NG, Tsai S, Christians KK, Clarke CN, Mogal H, et al. Transarterial chemoembolization in hepatocellular carcinoma with portal vein tumor thrombosis: a systematic review and meta-analysis. HPB (Oxford) 2017;19:659−666.ArticlePubMed
- 20. Liu L, Chen H, Wang M, Zhao Y, Cai G, Qi X, et al. Combination therapy of sorafenib and TACE for unresectable HCC: a systematic review and meta-analysis. PLoS One 2014;9:e91124. ArticlePubMedPMC
- 21. Chao Y, Chung YH, Han G, Yoon JH, Yang J, Wang J, et al. The combination of transcatheter arterial chemoembolization and sorafenib is well tolerated and effective in Asian patients with hepatocellular carcinoma: final results of the START trial. Int J Cancer 2015;136:1458−1467.ArticlePubMed
- 22. Yu JI, Park HC, Lim DH, Park WY. Predictive factors for Child-Pugh score elevation in hepatocellular carcinoma patients treated with conformal radiation therapy: dose-volume histogram analysis. Tumori 2013;99:164−171.ArticlePubMed
- 23. Oh D, Lim DH, Park HC, Paik SW, Koh KC, Lee JH, et al. Early three-dimensional conformal radiotherapy for patients with unresectable hepatocellular carcinoma after incomplete transcatheter arterial chemoembolization: a prospective evaluation of efficacy and toxicity. Am J Clin Oncol 2010;33:370−375.ArticlePubMed
- 24. Lawrence TS, Ten Haken RK, Kessler ML, Robertson JM, Lyman JT, Lavigne ML, et al. The use of 3-D dose volume analysis to predict radiation hepatitis. Int J Radiat Oncol Biol Phys 1992;23:781−788.ArticlePubMed
- 25. Nakazawa T, Hidaka H, Shibuya A, Okuwaki Y, Tanaka Y, Takada J, et al. Overall survival in response to sorafenib versus radiotherapy in unresectable hepatocellular carcinoma with major portal vein tumor thrombosis: propensity score analysis. BMC Gastroenterol 2014;14:84. ArticlePubMedPMC
- 26. Kim TH, Park JW, Kim BH, Kim H, Moon SH, Kim SS, et al. Does risk-adapted proton beam therapy have a role as a complementary or alternative therapeutic option for hepatocellular carcinoma? Cancers (Basel) 2019;11:230. ArticlePubMedPMC
- 27. Lu XJ, Dong J, Ji LJ, Luo JH, Cao HM, Xiao LX, et al. Safety and efficacy of TACE and gamma knife on hepatocellular carcinoma with portal vein invasion. Gut 2016;65:715−716.ArticlePubMed
- 28. Akahane M, Koga H, Kato N, Yamada H, Uozumi K, Tateishi R, et al. Complications of percutaneous radiofrequency ablation for hepato-cellular carcinoma: imaging spectrum and management. Radiographics 2005;25(Suppl 1): S57−S68.ArticlePubMed
- 29. Giorgio A, Calisti G, Montesarchio L, Scognamiglio U, Matteucci P, Coppola C, et al. Hepatocellular carcinoma invading portal venous system in cirrhosis: long-term results of percutaneous radiofrequency ablation of both the nodule and portal vein tumor thrombus. A case control study. Anticancer Res 2014;34:6785−6790.PubMed
- 30. Giorgio A, Di Sarno A, de Stefano G, Farella N, Scognamiglio U, de Stefano M, et al. Hepatocellular carcinoma with cirrhosis: are patients with neoplastic main portal vein invasion eligible for percutaneous radiofrequency ablation of both the nodule and the portal venous tumor thrombus? AJR Am J Roentgenol 2009;193:948−954.ArticlePubMed
- 31. Memon K, Kulik L, Lewandowski RJ, Mulcahy MF, Benson AB, Ganger D, et al. Radioembolization for hepatocellular carcinoma with portal vein thrombosis: impact of liver function on systemic treatment options at disease progression. J Hepatol 2013;58:73−80.ArticlePubMed
- 32. Edeline J, Crouzet L, Campillo-Gimenez B, Rolland Y, Pracht M, Guillygomarc’h A, et al. Selective internal radiation therapy compared with sorafenib for hepatocellular carcinoma with portal vein thrombosis. Eur J Nucl Med Mol Imaging 2016;43:635−643.ArticlePubMed
- 33. de la Torre MA, Buades-Mateu J, de la Rosa PA, Lué A, Bustamante FJ, Serrano MT, et al. A comparison of survival in patients with hepatocellular carcinoma and portal vein invasion treated by radioembolization or sorafenib. Liver Int 2016;36:1206−1212.ArticlePubMed
- 34. Vilgrain V, Pereira H, Assenat E, Guiu B, Ilonca AD, Pageaux GP, et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): an open-label randomised controlled phase 3 trial. Lancet Oncol 2017;18:1624−1636.PubMed
- 35. Chow PKH, Gandhi M, Tan SB, Khin MW, Khasbazar A, Ong J, et al. SIRveNIB: selective internal radiation therapy versus sorafenib in Asia-Pacific patients with hepatocellular carcinoma. J Clin Oncol 2018;36:1913−1921.PubMed
- 36. Itamoto T, Nakahara H, Tashiro H, Haruta N, Asahara T, Naito A, et al. Hepatic arterial infusion of 5-fluorouracil and cisplatin for unresectable or recurrent hepatocellular carcinoma with tumor thrombus of the portal vein. J Surg Oncol 2002;80:143−148.ArticlePubMed
- 37. Song DS, Song MJ, Bae SH, Chung WJ, Jang JY, Kim YS, et al. A comparative study between sorafenib and hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis. J Gastroenterol 2015;50:445−454.ArticlePubMed
- 38. Chan SL, Chong CC, Chan AW, Poon DM, Chok KS. Management of hepatocellular carcinoma with portal vein tumor thrombosis: review and update at 2016. World J Gastroenterol 2016;22:7289−7300.ArticlePubMedPMC
- 39. Chok KS, Cheung TT, Chan SC, Poon RT, Fan ST, Lo CM. Surgical outcomes in hepatocellular carcinoma patients with portal vein tumor thrombosis. World J Surg 2014;38:490−496.ArticlePubMed
- 40. Zhang YF, Le Y, Wei W, Zou RH, Wang JH, OuYang HY, et al. Optimal surgical strategy for hepatocellular carcinoma with portal vein tumor thrombus: a propensity score analysis. Oncotarget 2016;7:38845−38856.ArticlePubMedPMC
- 41. Peng BG, He Q, Li JP, Zhou F. Adjuvant transcatheter arterial chemoembolization improves efficacy of hepatectomy for patients with hepatocellular carcinoma and portal vein tumor thrombus. Am J Surg 2009;198:313−318.ArticlePubMed
- 42. Ye JZ, Wang YY, Bai T, Chen J, Xiang BD, Wu FX, et al. Surgical resection for hepatocellular carcinoma with portal vein tumor thrombus in the Asia-Pacific region beyond the Barcelona Clinic Liver Cancer treatment algorithms: a review and update. Oncotarget 2017;8:93258−93278.ArticlePubMedPMC
- 43. Pracht M, Edeline J, Lenoir L, Latournerie M, Mesbah H, Audrain O, et al. Lobar hepatocellular carcinoma with ipsilateral portal vein tumor thrombosis treated with yttrium-90 glass microsphere radio-embolization: preliminary results. Int J Hepatol 2013;2013:827649. ArticlePubMedPMC
- 44. Lee HS, Choi GH, Choi JS, Kim KS, Han KH, Seong J, et al. Surgical resection after down-staging of locally advanced hepatocellular carcinoma by localized concurrent chemoradiotherapy. Ann Surg Oncol 2014;21:3646−3653.ArticlePubMed
- 45. Lee KW, Suh SW, Choi Y, Jeong J, Yi NJ, Kim H, et al. Macrovascular invasion is not an absolute contraindication for living donor liver transplantation. Liver Transpl 2017;23:19−27.ArticlePubMed
- 46. Jeong Y, Shin MH, Yoon SM, Song GW, Kim KH, Ahn CS, et al. Liver transplantation after transarterial chemoembolization and radiotherapy for hepatocellular carcinoma with vascular invasion. J Gastrointest Surg 2017;21:275−283.ArticlePubMed
- 47. Choi JY, Yu JI, Park HC, Kwon CH, Kim JM, Joh JW, et al. The possibility of radiotherapy as downstaging to living donor liver transplantation for hepatocellular carcinoma with portal vein tumor thrombus. Liver Transpl 2017;23:545−551.ArticlePubMed
- 48. Soin AS, Bhangui P, Kataria T, Baijal SS, Piplani T, Gautam D, et al. Experience with LDLT in patients with hepatocellular carcinoma and portal vein tumor thrombosis postdownstaging. Transplantation 2020;104:2334−2345.ArticlePubMed
- 49. Mannina EM, Cardenes HR, Lasley FD, Goodman B, Zook J, Althouse S, et al. Role of stereotactic body radiation therapy before orthotopic liver transplantation: retrospective evaluation of pathologic response and outcomes. Int J Radiat Oncol Biol Phys 2017;97:931−938.ArticlePubMed
- 50. O’Connor JK, Trotter J, Davis GL, Dempster J, Klintmalm GB, Goldstein RM. Long-term outcomes of stereotactic body radiation therapy in the treatment of hepatocellular cancer as a bridge to transplantation. Liver Transpl 2012;18:949−954.ArticlePubMed
- 51. Levi Sandri GB, Ettorre GM, Colasanti M, De Werra E, Mascianà G, Ferraro D, et al. Hepatocellular carcinoma with macrovascular invasion treated with yttrium-90 radioembolization prior to transplantation. Hepatobiliary Surg Nutr 2017;6:44−48.ArticlePubMedPMC
- 52. Han DH, Joo DJ, Kim MS, Choi GH, Choi JS, Park YN, et al. Living donor liver transplantation for advanced hepatocellular carcinoma with portal vein tumor thrombosis after concurrent chemoradiation therapy. Yonsei Med J 2016;57:1276−1281.ArticlePubMedPMC
- 53. Schwacha-Eipper B, Minciuna I, Banz V, Dufour JF. Immunotherapy as a downstaging therapy for liver transplantation. Hepatology 2020;72:1488−1490.ArticlePubMed
- 54. Gassmann D, Weiler S, Mertens JC, Reiner CS, Vrugt B, Nägeli M, et al. Liver allograft failure after nivolumab treatment-a case report with systematic literature research. Transplant Direct 2018;4:e376. ArticlePubMedPMC
- 55. Heimbach JK, Kulik LM, Finn RS, Sirlin CB, Abecassis MM, Roberts LR, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018;67:358−380.ArticlePubMed
- 56. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2018;69:182−236.ArticlePubMed
References
Figure & Data
References
Citations
- Metastatic papillary renal cell carcinoma with portal vein tumor thrombosis confirmed on blind liver biopsy
Hun Kim, Tae Hoon Roh, Jun Seop Lee, Min Seong Kim, Beom Kyung Kim
Journal of Liver Cancer.2024; 24(1): 113. CrossRef - Refining MRI-based criteria for portal vein invasion in hepatocellular carcinoma: improving sensitivity beyond portal vein tumor thrombosis
Jeongju Kim, Woo Kyoung Jeong, Jong Man Kim, Sang Yun Ha, Kyunga Kim
Abdominal Radiology.2023; 49(2): 437. CrossRef - Prediction models of hepatocellular carcinoma recurrence after liver transplantation: A comprehensive review
Sang Jin Kim, Jong Man Kim
Clinical and Molecular Hepatology.2022; 28(4): 739. CrossRef
 PubReader
PubReader ePub Link
ePub Link Download Citation
Download Citation
- Download Citation
- Close
- Related articles
-
- Intermediate-stage hepatocellular carcinoma: refining substaging or shifting paradigm?
- Liver resection in selective hepatocellular carcinoma with Vp3 or Vp4 portal vein tumor thrombosis improves prognosis
- Comparison of atezolizumab plus bevacizumab and lenvatinib for hepatocellular carcinoma with portal vein tumor thrombosis
- Metastatic papillary renal cell carcinoma with portal vein tumor thrombosis confirmed on blind liver biopsy
- Sonazoid contrast-enhanced ultrasonography for the diagnosis of hepatocellular carcinoma: strengths and shortcomings

 Follow JLC on Twitter
Follow JLC on Twitter