 E-submission
E-submission
Search
- Page Path
- HOME > Search
Review Article
- A multidisciplinary approach with immunotherapies for advanced hepatocellular carcinoma
- Yu Rim Lee
- J Liver Cancer. 2023;23(2):316-329. Published online September 22, 2023
- DOI: https://doi.org/10.17998/jlc.2023.09.04

- 1,582 Views
- 103 Downloads
- 2 Citations
-
 Abstract
Abstract
 PDF
PDF - Hepatocellular carcinoma (HCC) is a highly aggressive disease that is usually diagnosed at an advanced stage. Advanced HCC has limited treatment options and often has a poor prognosis. For the past decade, tyrosine kinase inhibitors have been the only treatments approved for advanced HCC that have shown overall survival (OS) benefits; however, but their clinical efficacy has been limited. Recent trials have demonstrated promising advancements in survival outcomes through immunotherapy-based treatments, such as combinations of immune checkpoint inhibitors (ICIs) with other ICIs, antiangiogenic drugs, and locoregional therapies. The atezolizumab-bevacizumab and durvalumab-tremelimumab (STRIDE) regimen has significantly improved survival rates as a first-line treatment and has become the new standard of care. Therefore, combined treatments for advanced HCC can result in better treatment outcomes owing to their synergistic effects, which requires a multidisciplinary approach. Ongoing studies are examining other therapeutic innovations that can improve disease control and OS rates. Despite improvements in the treatment of advanced HCC, further studies on the optimal treatment selection and sequences, biomarker identification, combination approaches with other therapies, and development of novel immunotherapy agents are required. This review presents the current treatment options and clinical data of the ICI-based combination immunotherapies for advanced HCC from a multidisciplinary perspective.
-
Citations
Citations to this article as recorded by
- Reduced-Dose or Discontinuation of Bevacizumab Might Be Considered after Variceal Bleeding in Patients with Hepatocellular Carcinoma Receiving Atezolizumab/Bevacizumab: Case Reports
Kyeong-Min Yeom, Young-Gi Song, Jeong-Ju Yoo, Sang Gyune Kim, Young Seok Kim
Medicina.2024; 60(1): 157. CrossRef - Hepatocellular Carcinoma: Advances in Systemic Therapy
Insija Ilyas Selene, Merve Ozen, Reema A. Patel
Seminars in Interventional Radiology.2024; 41(01): 056. CrossRef
- Reduced-Dose or Discontinuation of Bevacizumab Might Be Considered after Variceal Bleeding in Patients with Hepatocellular Carcinoma Receiving Atezolizumab/Bevacizumab: Case Reports

Original Article
- Clinical outcome of surgical resection for multifocal T2-T3 hepatocellular carcinoma up to 3 nodules: a comparative analysis with a single nodule
- Sehyeon Yu, Hye-Sung Jo, Young-Dong Yu, Yoo jin Choi, Dong-Sik Kim
- J Liver Cancer. 2023;23(2):377-388. Published online September 15, 2023
- DOI: https://doi.org/10.17998/jlc.2023.08.24
- 648 Views
- 35 Downloads
-
Abstract
PDF
 Supplementary Material
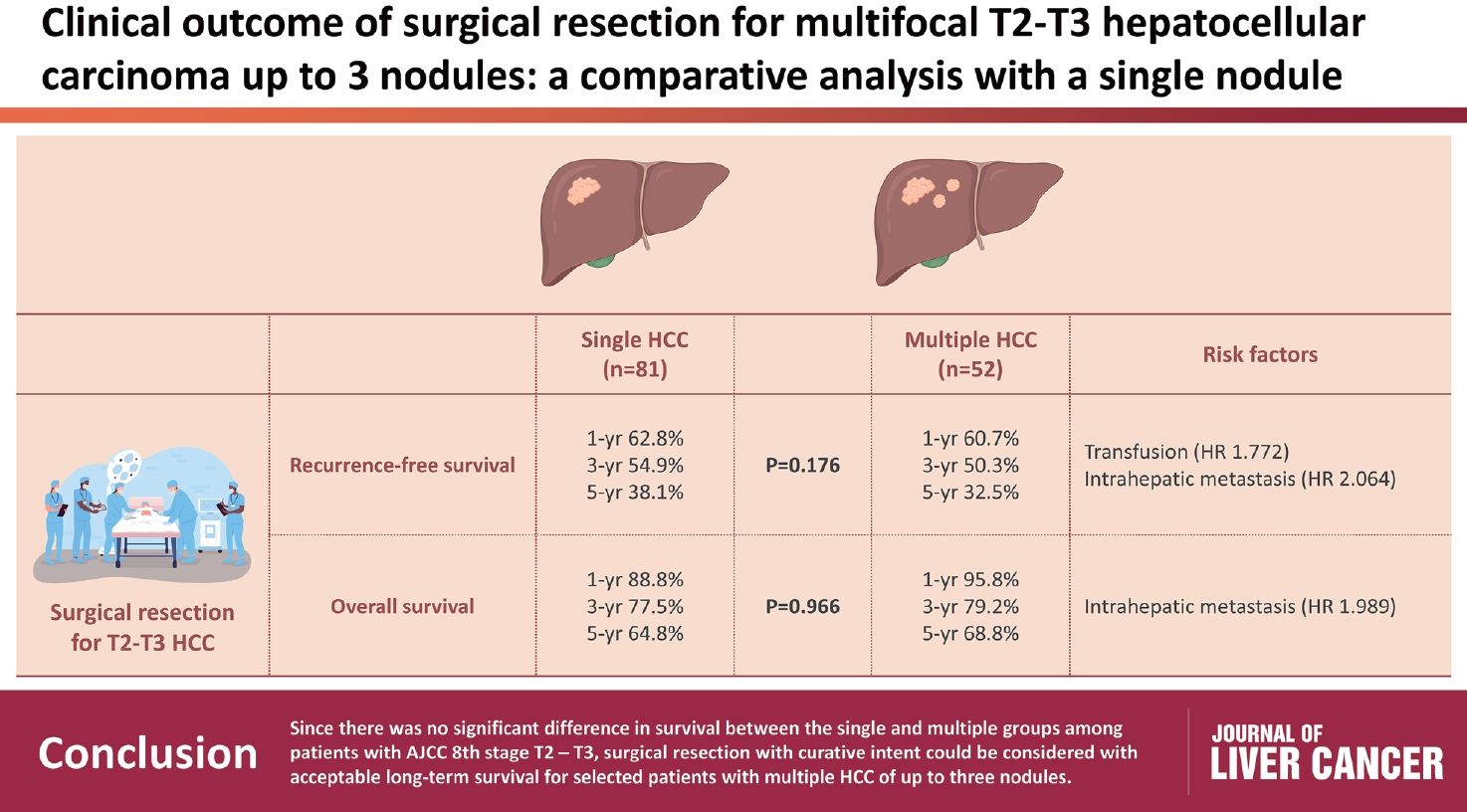
Supplementary Material - Background/Aim
s: Although the Barcelona Clinic Liver Cancer staging system seems to underestimate the impact of curative-intent surgical resection for multifocal hepatocellular carcinoma (HCC), recent studies have indicated favorable results for the surgical resection of multiple HCC. This study aimed to assess clinical outcomes and feasibility of surgical resection for multifocal HCC with up to three nodules compared with single tumor cases.
Methods
Patients who underwent surgical resection for HCC with up to three nodules between 2009 and 2020 were included, and those with the American Joint Committee on Cancer (AJCC) 8th edition, T1 and T4 stages were excluded to reduce differences in disease distribution and severity. Finally, 81 and 52 patients were included in the single and multiple treatment groups, respectively. Short- and long-term outcomes including recurrence-free survival (RFS) and overall survival (OS), were evaluated.
Results
All patients were classified as Child-Pugh class A. RFS and OS were not significantly different between the two groups (P=0.176 and P=0.966, respectively). Multivariate analysis revealed that transfusion and intrahepatic metastasis were significantly associated with recurrence (P=0.046 and P=0.005, respectively). Additionally, intrahepatic metastasis was significantly associated with OS (hazard ratio, 1.989; 95% confidence interval, 1.040-3.802; P=0.038).
Conclusions
Since there was no significant difference in survival between the single and multiple groups among patients with AJCC 8th stage T2 and T3, surgical resection with curative intent could be considered with acceptable long-term survival for selected patients with multiple HCC of up to three nodules.
Review Article
- Non-alcoholic fatty liver disease-related hepatocellular carcinoma
- Darine Daher, Karim Seif El Dahan, Amit G. Singal
- J Liver Cancer. 2023;23(1):127-142. Published online February 9, 2023
- DOI: https://doi.org/10.17998/jlc.2022.12.30
- 3,259 Views
- 169 Downloads
- 7 Citations
-
Abstract
PDF
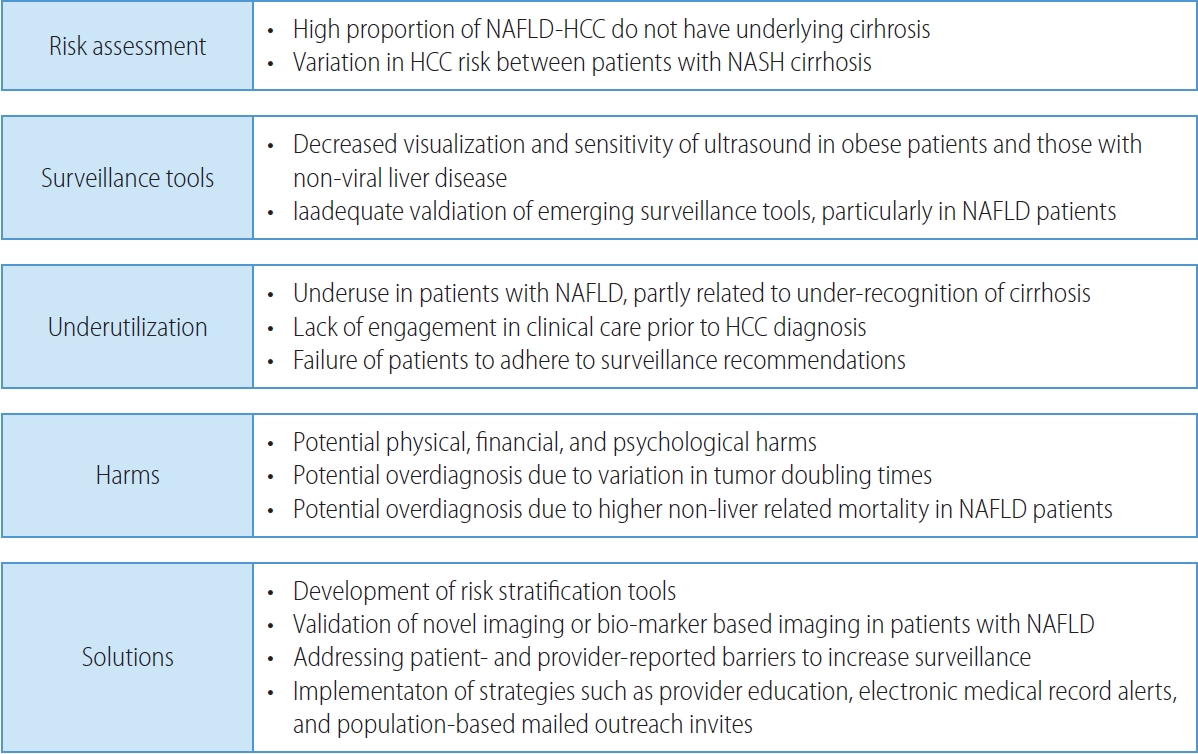
- Non-alcoholic fatty liver disease (NAFLD), one of the most common causes of liver disease, is an increasingly common cause of hepatocellular carcinoma (HCC). Several demographic, clinical, and genetic factors contribute to HCC risk in NAFLD patients, which may inform risk stratification scores. Proven efficacious approaches to primary prevention approach in patients with non-viral liver disease remain an area of need. Semi-annual surveillance is associated with improved early tumor detection and reduced HCC-related mortality; however, patients with NAFLD have several challenges to effective surveillance, including under-recognition of at-risk patients, low surveillance utilization in clinical practice, and lower sensitivity of current tools for early-stage HCC detection. Treatment decisions are best made in a multidisciplinary fashion and are informed by several factors including tumor burden, liver dysfunction, performance status, and patient preferences. Although patients with NAFLD often have larger tumor burden and increased comorbidities compared to counterparts, they can achieve similar post-treatment survival with careful patient selection. Therefore, surgical therapies continue to provide a curative treatment option for patients diagnosed at an early stage. Although there has been debate about the efficacy of immune checkpoint inhibitors in patients with NAFLD, current data are insufficient to change treatment selection based on liver disease etiology.
-
Citations
Citations to this article as recorded by- Overnutrition and Lipotoxicity: Impaired Efferocytosis and Chronic Inflammation as Precursors to Multifaceted Disease Pathogenesis
Vivek Mann, Alamelu Sundaresan, Shishir Shishodia
Biology.2024; 13(4): 241. CrossRef - Risk of Hepatocellular Carcinoma by Steatotic Liver Disease and Its Newly Proposed Subclassification
Byeong Geun Song, Aryoung Kim, Myung Ji Goh, Wonseok Kang, Geum-Youn Gwak, Yong-Han Paik, Moon Seok Choi, Joon Hyeok Lee, Dong Hyun Sinn
Liver Cancer.2024; : 1. CrossRef - Smoking Increases the Risk of Hepatocellular Carcinoma and Cardiovascular Disease in Patients with Metabolic-Associated Fatty Liver Disease
Jeong-Ju Yoo, Man Young Park, Eun Ju Cho, Su Jong Yu, Sang Gyune Kim, Yoon Jun Kim, Young Seok Kim, Jung-Hwan Yoon
Journal of Clinical Medicine.2023; 12(9): 3336. CrossRef - Reply: Validation of MELD 3.0 scoring system in East Asian patients with cirrhosis awaiting liver transplantation
Jeong-Ju Yoo, Sang Gyune Kim
Liver Transplantation.2023; 29(11): E38. CrossRef - Unraveling the Janus-Faced Role of Autophagy in Hepatocellular Carcinoma: Implications for Therapeutic Interventions
Thi Ha Nguyen, Tuan Minh Nguyen, Dinh Thi Minh Ngoc, Taesik You, Mi Kyung Park, Chang Hoon Lee
International Journal of Molecular Sciences.2023; 24(22): 16255. CrossRef - Comparative Analysis of Atezolizumab Plus Bevacizumab and Hepatic Artery Infusion Chemotherapy in Unresectable Hepatocellular Carcinoma: A Multicenter, Propensity Score Study
Ji Kim, Hee-Chul Nam, Chang-Wook Kim, Hee Cho, Jae-Sung Yoo, Ji Han, Jeong Jang, Jong Choi, Seung Yoon, Hyun Yang, Si Bae, Suho Kim, Jung Oh, Ho Chun, Chang Jeon, Jaegyoon Ahn, Pil Sung
Cancers.2023; 15(17): 4233. CrossRef - A nationwide study on the current treatment status and natural prognosis of hepatocellular carcinoma in elderly
Jeong-Ju Yoo, Jayoun Lee, Gi Hong Choi, Min Woo Lee, Dong Ah Park
Scientific Reports.2023;[Epub] CrossRef
- Overnutrition and Lipotoxicity: Impaired Efferocytosis and Chronic Inflammation as Precursors to Multifaceted Disease Pathogenesis
Case Report
- Multidisciplinary treatment with immune checkpoint inhibitors for advanced stage hepatocellular carcinoma
- Ahlim Lee, Jaejun Lee, Hyun Yang, Soo-Yoon Sung, Chang Ho Jeon, Su Ho Kim, Moon Hyung Choi, Young Joon Lee, Ho Jong Chun, Si Hyun Bae
- J Liver Cancer. 2022;22(1):75-83. Published online March 18, 2022
- DOI: https://doi.org/10.17998/jlc.2022.03.04
- 3,989 Views
- 93 Downloads
- 3 Citations
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) is a cytotoxic chemotherapy-resistant tumor and most HCCs arise in a background of liver cirrhosis of various causes. Although the IMBrave150 trial showed remarkable advancements in the treatment of unresectable HCC with atezolizumab plus bevacizumab (AteBeva), therapeutic outcomes were unsatisfactory in more than half of the patients. Accordingly, many ongoing trials combine conventional modalities with new drugs such as immune checkpoint inhibitors for better treatment outcomes, and they are expected to benefit patients with limited responses to conventional treatment. Here, two patients with advanced stage HCC with preserved liver function and good performance status showed partial response after treatment with combination or sequential therapy of AteBeva, hepatic arterial infusion chemotherapy, radiation therapy, and transarterial chemoembolization. These findings indicate the efficacy of multidisciplinary treatment against advanced HCC. Additional studies are required to establish optimal treatment strategies.
-
Citations
Citations to this article as recorded by- Complications of immunotherapy in advanced hepatocellular carcinoma
Young-Gi Song, Jeong-Ju Yoo, Sang Gyune Kim, Young Seok Kim
Journal of Liver Cancer.2024; 24(1): 9. CrossRef - Feasibility of additional radiotherapy in patients with advanced hepatocellular carcinoma treated with atezolizumab plus bevacizumab
Tae Hyun Kim, Bo Hyun Kim, Yu Ri Cho, Young-Hwan Koh, Joong-Won Park
Journal of Liver Cancer.2023; 23(2): 330. CrossRef - Is multidisciplinary treatment effective for hepatocellular carcinoma with portal vein tumor thrombus?
Won Hyeok Choe
Journal of Liver Cancer.2022; 22(1): 1. CrossRef
- Complications of immunotherapy in advanced hepatocellular carcinoma
Review Articles
- External Beam Radiotherapy for Hepatocellular Carcinoma: a Review of the Current Guidelines in the East and the West
- Sang Min Yoon
- J Liver Cancer. 2021;21(1):25-33. Published online March 31, 2021
- DOI: https://doi.org/10.17998/jlc.21.1.25
- 4,110 Views
- 157 Downloads
- 4 Citations
-
Abstract
PDF
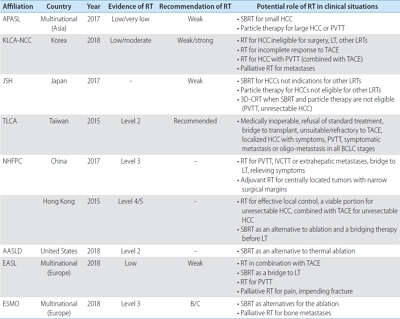
- The incidence of hepatocellular carcinoma (HCC) is geographically heterogeneous depending on the underlying liver disease. Moreover, the decisions and recommendations about standard treatments differ between countries, especially between the East and the West. Because of the complexity of treatment decisions for the management of HCC, a multidisciplinary approach is recommended to maximize the therapeutic efficacy. External beam radiotherapy (RT) has been increasingly used to manage HCC when recommended treatments cannot be applied in real-world clinical practice. However, Western guidelines for the management of HCC do not recommend RT as a treatment option due to the lack of clinical evidence. RT has often been used more in Eastern countries than in Western countries; hence, it is necessary to review both Eastern and Western guidelines for HCC treatment regarding the recommendations about RT. In this study, the comments and potential roles of external beam RT are summarized from several treatment guidelines for the management of HCC.
-
Citations
Citations to this article as recorded by- Concurrent nivolumab and external beam radiation therapy for hepatocellular carcinoma with macrovascular invasion: A phase II study
Bo Hyun Kim, Hee Chul Park, Tae Hyun Kim, Young-Hwan Koh, Jung Yong Hong, Yuri Cho, Dong Hyun Sinn, Boram Park, Joong-Won Park
JHEP Reports.2024; 6(4): 100991. CrossRef - Novel paradigm in the treatment of hepatocellular carcinoma: Anticipating breakthroughs with particle therapy
Sang Min Yoon
Clinical and Molecular Hepatology.2023; 29(4): 977. CrossRef - Loco-regional therapies competing with radiofrequency ablation in potential indications for hepatocellular carcinoma: a network meta-analysis
Ha Il Kim, Jihyun An, Seungbong Han, Ju Hyun Shim
Clinical and Molecular Hepatology.2023; 29(4): 1013. CrossRef - Differences in radiotherapy application according to regional disease characteristics of hepatocellular carcinoma
Chai Hong Rim
Journal of Liver Cancer.2021; 21(2): 113. CrossRef
- Concurrent nivolumab and external beam radiation therapy for hepatocellular carcinoma with macrovascular invasion: A phase II study
- Locoregional Treatment of Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis
- Sang Youn Hwang, Ryoung-Go Kim, Cheol-Won Choi, Sang Bu Ahn
- J Liver Cancer. 2016;16(2):69-81. Published online September 30, 2016
- DOI: https://doi.org/10.17998/jlc.16.2.69
- 1,001 Views
- 10 Downloads
- 1 Citation
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) patients with portal vein tumor thrombosis (PVTT) have a extremely poor prognosis. According to the Barcelona Clinic Liver Cancer guideline, sorafenib is a standard therapy in this situation, but many clinicians still select locoregional therapy (LRT) such as transarterial therapy, external beam radiation therapy (EBRT), even surgical resection (SR) or combination of LRTs because the survival improvement by sorafenib is unsatisfactory. Based on recent meta-analysis and prospective study, transarterial chemoembolization (TACE) and transarterial radioembolization seem to be effective and safe therapeutic option that have comparable outcome to sorafenib. Recently large nationwide studies demonstrated that SR can be a potentially curative treatment in selected patients. Hepatic arterial infusion chemotherapy (HAIC) can be also good option, especially in Child class B patients based on small volume prospective studies. Moreover, multidisciplinary strategies based on the combination of LRTs (SR plus TACE, TACE + EBRT, TACE + Sorafenib, HAIC + EBRT etc.) may improve survival of HCC patients with PVTT. Finally we discuss individualized and tailored treatment strategies for different clinical situations.
-
Citations
Citations to this article as recorded by- Progress in Non-Surgical Treatment of Primary Hepatocellular Carcinoma with Combined Portal Vein Carcinoma Thrombosis
文豪 寇
Advances in Clinical Medicine.2023; 13(07): 11779. CrossRef
- Progress in Non-Surgical Treatment of Primary Hepatocellular Carcinoma with Combined Portal Vein Carcinoma Thrombosis
Case Reports
- Regression of Advanced Hepatocellular Carcinoma with Lung Metastasis in Response to Sorafenib
- Dae-ha Kim, Gee ho Min, Dong-won Lee, Ke Ryun Ahn, Ji Hye Kim, Snag-Jun Suh, Young Kul Jung, Hyung Joon Yim
- J Liver Cancer. 2016;16(1):57-62. Published online March 31, 2016
- DOI: https://doi.org/10.17998/jlc.16.1.57
- 1,054 Views
- 6 Downloads
-
Abstract
PDF
- Sorafenib is a multi-targeted tyrosine kinase inhibitor that inhibits Raf kinase and the vascular endothelial growth factor receptor intracellular kinase pathway and is the first agent to demonstrate a statistically significant improvement in overall survival for patients with advanced hepatocellular carcinoma (HCC). However, there were few cases of partial or complete response reported in the previous studies. We herein report a case of dramatic partial response in a patient who had advanced HCC with multiple lung metastasis and portal vein thrombosis treated with sorafenib.
- A Case of Hepatocellular Carcinoma with Improved Decompansated Liver Cirrhosis with Combination Treatment of Transarterial Chemoembolization and Radiofrequency Ablation
- Hyung Min Yu, Won Hyeok Choe, So Young Kwon, Jeong Han Kim
- J Liver Cancer. 2014;14(2):131-134. Published online September 30, 2014
- DOI: https://doi.org/10.17998/jlc.14.2.131
- 1,077 Views
- 5 Downloads
-
Abstract
PDF
- A 54-year-old female patient with no medical history visited our hospital complaining of both pretibial pitting oedema for 6 months, and abdominal distension for 1 month. Computed tomography and magnetic resonance imaging revealed an 2.3cm sized tumour at segment 2 of the liver. Her Child-Turcotte-Pugh (CTP) class was C (score 11) at the initial visit. She was diagnosed as hepatocellular carcinoma (UICC stage II, BCLC stage D), and then she underwent conservative treatment for 1 month. After one month of conservative treatment, her liver function was improved to CTP class B (score 8), and then she underwent combination treatment of transarterial chemoembolization and radiofrequency ablation. However, her liver function was deteriorated gradually. She was transferred to other hospital for liver transplantation eventually. (J Liver Cancer 2014;14:131-134)
Review Articles
- Directions for Future Hepatocellular Carcinoma Treatment Guidelines; Hepatologist’s Perspective: Systemic Approach to Multidisciplinary Treatment
- Soo Young Park, Won Young Tak
- Journal of the Korean Liver Cancer Study Group. 2013;13(1):8-13. Published online February 28, 2013
- DOI: https://doi.org/10.17998/jlc.13.1.8
- 961 Views
- 5 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma is one of the most important malignancies in Korea with high mortality rates. Although current guidelines define treatment algorithm by performance status, underlying liver function, size and number of hepatocellular carcinoma, those are not fully reflect the complexities of patients’ characteristics and recently advanced available therapeutic options. Treatment can be optimized by available therapeutic options based on the patients’ characteristics. Because of the heterogeneity in presentation among patients, it is now widely accepted that management of hepatocellular carcinoma requires multimodality and multidisciplinary treatment approaches involving hepatologists, surgeons, interventional radiologists, and radiation oncologists. These approaches are important in improving the survival of patients with hepatocellular carcinoma.
- Treatment Response Evaluation of Hepatocellular Carcinoma
- Joon-Il Choi
- Journal of the Korean Liver Cancer Study Group. 2012;12(1):16-22. Published online February 28, 2012
- 490 Views
- 0 Download
-
Abstract
PDF
- The most important and primary endpoint in oncology research is overall survival. However, other endpoints such as time-to-progression, time-to-recurrence and response rate have their roles in oncology trials and these endpoints are assessed by the imaging evaluation of tumor burden. Recently published the revised version (version 1.1) of response evaluation criteria in solid tumors (RECIST) is now the standards for the tumor response evaluation after treatment, and especially for cytotoxic agents. However, the problems are more complicated for hepatocellular carcinoma (HCC). RECIST are mainly used for the response evaluation of chemotherapeutic agents. However, for the treatment of HCC, there are some locoregional treatments and molecular targeted agents, and after these treatments, tumor necrosis remains as non-enhanced tumor areas, whereas viable tumor parts can be noted by the enhanced areas. However, these necrotic areas should be included as being tumor when we adopt the pure anatomical criteria such as RECIST and this can distort the results of the response evaluation. For overcoming this problem, some new criteria were introduced and their principle is the measurement of enhancing portion of the tumor only. However, these new criteria still have limitations and functional imaging is thought to be the future problem-solving tool for the evaluation of response for molecular targeted agents.
Case Reports
- Two Cases of Small (< 1 cm) Hepatocellular Carcinoma
- Jin Yong Jung, Sun Young Yim, Chang Ha Kim, Jin Dong Kim, Yeon Seok Seo, Hyung Joon Yim, Ho Sang Ryu, Min Ju Kim, Beom Jin Park, Soon Ho Um
- Journal of the Korean Liver Cancer Study Group. 2012;12(1):37-41. Published online February 28, 2012
- 515 Views
- 2 Downloads
-
Abstract
PDF
- Tumor size is one of the most important factors for decision of therapeutic plan and prognosis of hepatocellular carcinoma (HCC). If the diagnosis of HCC is made earlier in its small size, the prognosis is better. However the diagnosis of small HCC is not easy because small HCC lacks the typical clinical and radiologic feature. We experienced two cases of small HCC less than 1 cm that was confirmed after first treatment.
- A Case of Small Hepatocellular Carcinoma Less Than 1 cm
- Yun Jeong Jo, Young Kul Jung, Dong Hae Chung, Oh Sang Kwon, Yun Soo Kim, Duck Joo Choi, Ju Hyun Kim
- Journal of the Korean Liver Cancer Study Group. 2012;12(1):42-46. Published online February 28, 2012
- 485 Views
- 1 Download
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) is one of the most important causes of cancer death in South Korea. Approximately two thirds of the patients are diagnosed in the advanced stage with multiple metastasis and underlying liver dysfunction, so they are not suitable to undergo curative resection. Small HCC has no consensus about diagnostic criteria but became known early stage HCC that means good prognosis. Cases of small HCC have been increasing with the progress of diagnostic methods. We experienced a case of incidentally found small HCC less than 1 cm from liver cirrhosis by liver dynamic imaging, so reported it.
Review Article
- Practice Guidelines for Management of Hepatocellular Carcinoma: Global Discrepancies and Solution of Local Ablation
- Hong Soo Kim
- Journal of the Korean Liver Cancer Study Group. 2011;11(1):6-11. Published online February 28, 2011
- 483 Views
- 1 Download
-
Abstract
PDF
- A curative modality for hepatocellular carcinoma was a resection or a liver transplantation in a past decades, but nowadays local ablation therapy like a percutaneous alcohol injection or a radiofrequency ablation is comparable with a surgical resection. So a local ablation therapy is considered as a curative modality. Recently early detection of a small hepatocellular carcinoma is becoming easy due to use a suveillance ultrasonography and computed tomography in a high risk patients. Grobally, an indication for local ablation therapy is a small hepatocellular carcinoma less than 3 cm in diameter and have a well-reserved liver function. But patients who met above indication is also controlled by a liver transplantation or a surgical resection. So we should pay attention to a difference between treatment guidelines and a strengths and weaknesses of local ablation therapy.
Case Reports
- A Case of Advanced Hepatocellular Carcinoma Treated with Curative Surgical Resection after Downstaging by Hepatic Arterial Infusion Chemotherapy
- Jong Ryul Eun, Heon Ju Lee, Jae Woon Kim, Jay Chun Chang, Sung Su Yun, Joon Hyuk Choi
- Journal of the Korean Liver Cancer Study Group. 2011;11(1):60-64. Published online February 28, 2011
- 511 Views
- 2 Downloads
-
Abstract
PDF
- Cure by single modality for advanced hepatocellular carcinoma (HCC) is difficult. Therefore, multidisciplinary approaches are needed to get a better outcome for advanced HCC. In this paper, we report a case of advanced HCC treated with curative surgical resection after downstaging by hepatic arterial infusion chemotherapy (HAIC). A 50-year-old male patient had a maximum 16.0 cm sized HCC in the right lobe. He achieved a partial response after 2 cycles of HAIC with 5-FU (750 mg/m2) and cisplatin (25 mg/m2). After completion of 6 cycles, he received a curative right hepatectomy and the histopathology revealed 95% of tumor necrosis. He is under follow-up without recurrence at 14 months of surgery. This case suggests that surgery after downstaging by HAIC may provide good clinical outcome in advanced HCC.
- A Case of Hepatocellular Carcinoma Who had Surgical Resection Following TACE and Sorafenib Chemotherapy
- Geum Youb Noh, Chul Ju Han, Youn Joo Kim, Ki Young Yang, Su Cheol Park, Jin Kim, Yu Cheol Kim, Yoon Hee Choi, Hyo Rak Lee
- Journal of the Korean Liver Cancer Study Group. 2011;11(1):65-68. Published online February 28, 2011
- 503 Views
- 0 Download
-
Abstract
PDF
- Surgical resection for hepatocellular carcinoma (HCC) is one of the managements, showing improved long term survival. Nowadays, it is being accepted as the main curative treatment. However, the biggest problem we used to face is that surgery cannot be applied at the point of presentation in many patients due to advanced stage. Here we present a case of 54 years old female, who had transarterial chemoembolization (TACE) and sorafenib due to advanced stage of HCC, and later underwent curative surgery due to remarkable response. She had a CT scan of abdomen, which showed multiple huge masses. HCC was confirmed by ultrasonography-guided liver biopsy. TACE was performed once. After TACE, the size of masses increased. Therefore, sorafenib was administered and then continued for 9 months. As partial response was obtained at that time, surgical resection was successfully done. In the pathological report of removed tumor, we could confirm total necrosis of tumor. Now, its been 6 months and she is followed up without any recurrence.
 First
First Prev
Prev


 Follow JLC on Twitter
Follow JLC on Twitter