 E-submission
E-submission
Search
- Page Path
- HOME > Search
Case Report
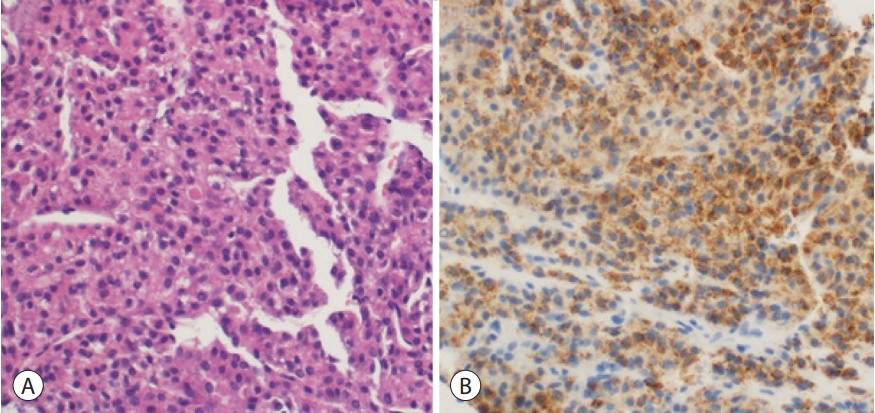
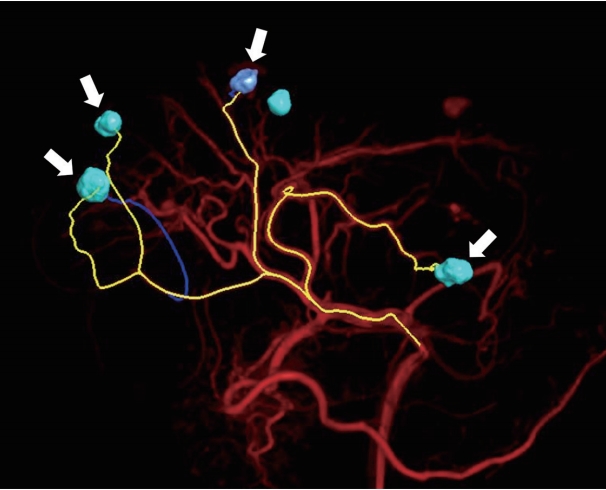
- Combination Therapy of Angiotherapy, Radiation Therapy, and Radiofrequency Ablation for Pulmonary Metastasis of Hepatocellular Carcinoma Accompanied by Nontuberculous Mycobacteria
- Sang Hyun Park, Seul Ki Kim, Ji Hye Kim, Seokgyo Seo, Hyun Pyo Hong, Soo-Youn Ham, Byung Ik Kim
- J Liver Cancer. 2019;19(1):79-84. Published online March 31, 2019
- DOI: https://doi.org/10.17998/jlc.19.1.79
- 3,288 Views
- 52 Downloads
-
 Abstract
Abstract
 PDF
PDF - With the advances in hepatocellular carcinoma (HCC) treatment, the lung metastasis of HCC is becoming increasingly important. In treating the lung metastasis of HCC, a multidisciplinary approach can lead to better results than systemic chemotherapy alone. Here, we report on a patient who presented with pulmonary masses, while the HCC was being controlled in the abdominal cavity. The presence of nontuberculous mycobacteria was identified during the diagnosis of the pulmonary masses. The pulmonary metastases of HCC were treated with a combination of angiotherapy, radiation therapy, and radiofrequency ablation. The patient showed a satisfactory progress with this multidisciplinary localized treatment. We report the clinical progress and review the recent literature regarding the treatment of pulmonary metastasis without intrahepatic HCC herein.

Review Articles
- Conventional Chemoembolization for Hepatocellular Carcinoma: Role of Cone-Beam Computed Tomography Guidance
- In Joon Lee, Jin Wook Chung
- J Liver Cancer. 2019;19(1):19-29. Published online March 31, 2019
- DOI: https://doi.org/10.17998/jlc.19.1.19
- 5,232 Views
- 145 Downloads
- 4 Citations
-
Abstract
PDF
- Conventional chemoembolization using Lipiodol-based regimens was introduced in the 1980s, and it is currently recommended as the primary treatment modality for patients with unresectable, intermediate, or locally advanced hepatocellular carcinoma (HCC) by the international guidelines. For better therapeutic efficacy and safety, chemoembolization should be performed as selectively as possible through tumor-feeding arteries, based on the detection of arterial supply to the HCC. With the technical advancement of flat-panel detector, cone-beam computed tomography (CBCT) is mounted on the C-arm of the angiographic machine. CBCT facilitates the detection of small occult HCCs and fine tumor-feeding arteries, recognition of extrahepatic collateral supply, navigation of a microcatheter to the target feeding arteries, prevention of non-target embolization, and intraprocedural assessment of the completeness of treatment with chemoembolization. These functions performed by CBCT ultimately improve the safety and efficacy of chemoembolization and may contribute to improving the prognosis of the patient with HCC.
-
Citations
Citations to this article as recorded by
- Transarterial Chemoembolization for Hepatocellular Carcinoma: 2023 Expert Consensus-Based Practical Recommendations of the Korean Liver Cancer Association
Yuri Cho, Jin Woo Choi, Hoon Kwon, Kun Yung Kim, Byung Chan Lee, Hee Ho Chu, Dong Hyeon Lee, Han Ah Lee, Gyoung Min Kim, Jung Suk Oh, Dongho Hyun, In Joon Lee, Hyunchul Rhim
Korean Journal of Radiology.2023; 24(7): 606. CrossRef - Transarterial chemoembolization for hepatocellular carcinoma: 2023 expert consensus-based practical recommendations of the Korean Liver Cancer Association
Yuri Cho, Jin Woo Choi, Hoon Kwon, Kun Yung Kim, Byung Chan Lee, Hee Ho Chu, Dong Hyeon Lee, Han Ah Lee, Gyoung Min Kim, Jung Suk Oh, Dongho Hyun, In Joon Lee, Hyunchul Rhim
Journal of Liver Cancer.2023; 23(2): 241. CrossRef - Transarterial chemoembolization for hepatocellular carcinoma: 2023 Expert consensus-based practical recommendations of the Korean Liver Cancer Association
Yuri Cho, Jin Woo Choi, Hoon Kwon, Kun Yung Kim, Byung Chan Lee, Hee Ho Chu, Dong Hyeon Lee, Han Ah Lee, Gyoung Min Kim, Jung Suk Oh, Dongho Hyun, In Joon Lee, Hyunchul Rhim
Clinical and Molecular Hepatology.2023; 29(3): 521. CrossRef - The efficacy of TACE; how can automated feeder software help?
Hassan Abdelsalam, Doaa M. Emara, Ehab M. Hassouna
Egyptian Journal of Radiology and Nuclear Medicine.2022;[Epub] CrossRef
- Transarterial Chemoembolization for Hepatocellular Carcinoma: 2023 Expert Consensus-Based Practical Recommendations of the Korean Liver Cancer Association
- Tumor Response Evaluation after Treatment and Post-treatment Surveillance of Hepatocellular Carcinoma
- Yoon, Jun Sik , Park, Soo Young
- J Liver Cancer. 2018;18(1):9-16. Published online March 31, 2018
- DOI: https://doi.org/10.17998/jlc.18.1.9
- 8,656 Views
- 209 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma is one of the most prevalent malignancies and frequent causes of death worldwide. Treatment options of hepatocellular carcinoma consist of locoregional therapy, surgical resection, liver transplantation, and systemic therapy. Assessment of tumor response is required in patients receiving locoregional and systemic therapy. The Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 is widely used tumor response evaluation criteria. However, the RECIST does not reflect the extent of tumor necrosis after some locoregional therapies and molecular targeted agents. The Modified RECIST (mRECIST), which has the concept of viable tumor, was introduced in order to overcome this problem. The mRECIST were developed on the basis of RECIST version 1.1 and only tumoral tissue showing contrast uptake in arterial phase of dynamic radiologic imaging techniques was measured to assess tumor response. Recently, immune checkpoint inhibitors have emerged as a promising therapeutic modality for the treatment of hepatocellular carcinoma. To identify tumor response after immunotherapy, immune RECIST (iRECIST) has been proposed as consensusbased criteria. After achieving complete response after curative treatment, optimal surveillance was needed to detect recurrence. Individualized surveillance schedule should be considered, taking into consideration the risk factors of the patient and the risk associated with the treatment modalities.
Case Report
- A Case of Advanced Hepatocellular Carcinoma with Long-term Post-progression Survival under Repeated Transarterial Chemoembolization after Sorafenib Failure
- Jihyun Lee, Hwi Young Kim, Yong Jin Jung, Tae Hun Kim, Kwon Yu
- J Liver Cancer. 2017;17(1):82-87. Published online March 31, 2017
- DOI: https://doi.org/10.17998/jlc.17.1.82
- 1,635 Views
- 8 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma is the third leading cause of cancer related mortality worldwide. Only 30% of patients are eligible for curative surgical resection at diagnosis. For patients with advanced hepatocellular carcinoma with accompanying portal vein tumor thrombosis, Sorafenib is recommended as first-line treatment. However, survival gain from sorafenib is unsatisfactory, and there is no standard therapy for patients who are intolerable or refractory to sorafenib. Here we report a case of a 52-year-old man who initially achieved partial response after sorafenib treatment, but eventually showed disease progression and was treated subsequently with transarterial chemoembolization (TACE). Multinodular recurrence occurred, but he was treated with repeated TACE, and has survived for 4 years so far.
 First
First Prev
Prev


 Follow JLC on Twitter
Follow JLC on Twitter