 E-submission
E-submission
Search
- Page Path
- HOME > Search
Original Article
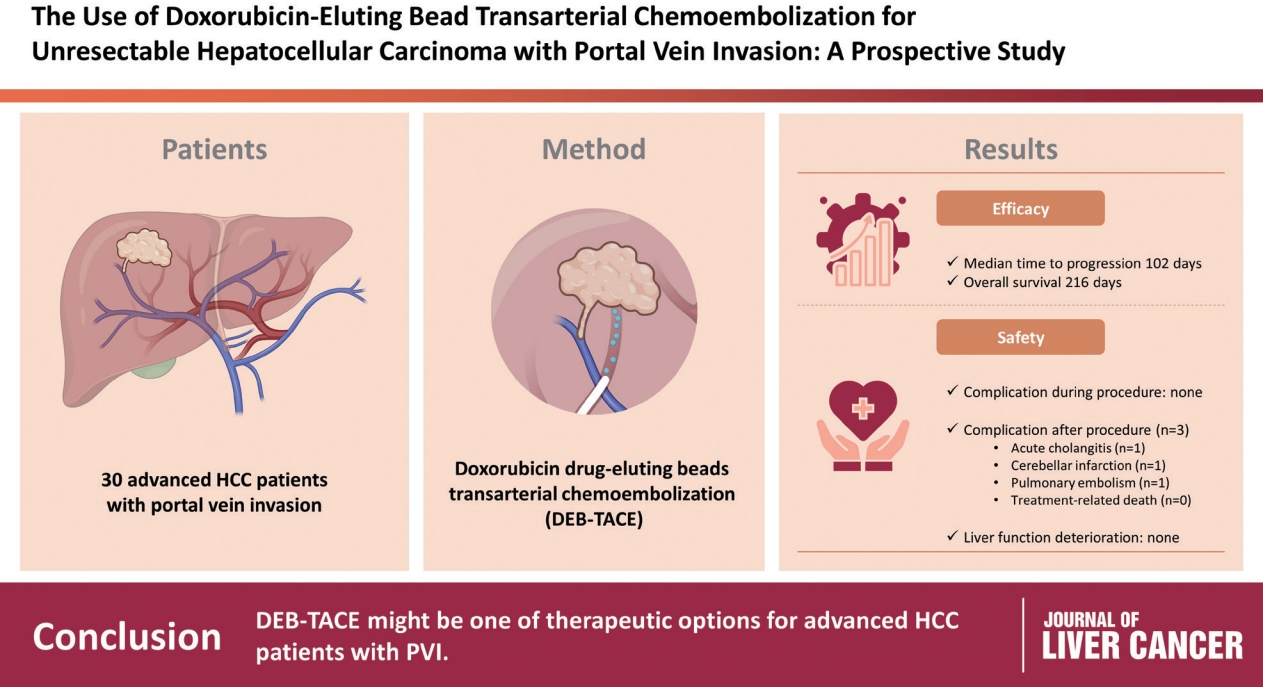
- Use of doxorubicin-eluting bead transarterial chemoembolization for unresectable hepatocellular carcinoma with portal vein invasion: a prospective study
- Su Jong Yu, Yun Bin Lee, Eun Ju Cho, Jeong-Hoon Lee, Hyo-Cheol Kim, Jin Wook Chung, Jung-Hwan Yoon, Yoon Jun Kim
- J Liver Cancer. 2023;23(1):166-176. Published online March 3, 2023
- DOI: https://doi.org/10.17998/jlc.2023.02.08
- 2,090 Views
- 95 Downloads
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Background/Aim
To evaluate the applicability of transarterial chemoembolization (TACE) treatment with doxorubicin drug-eluting beads (DEBs) in advanced hepatocellular carcinoma (HCC) patients with portal vein invasion (PVI).
Methods
This prospective study was approved by the institutional review board and informed consent was obtained from all participants. A total of 30 HCC patients with PVI received DEB-TACE between 2015 and 2018. The following parameters were evaluated: complications during DEB-TACE, abdominal pain, fever, and laboratory outcomes, including liver function change. Overall survival (OS), time to progression (TTP), and adverse events were also analyzed and assessed.
Results
DEBs measuring 100–300 μm in diameter were loaded with doxorubicin (150 mg per procedure). There were no complications during DEB-TACE and no significant differences in the levels of prothrombin time, serum albumin, or total bilirubin at follow-up compared to baseline. The median TTP was 102 days (95% confidence interval [CI], 42–207 days) and the median OS was 216 days (95% CI, 160–336 days). Three patients (10%) had severe adverse reactions, including transient acute cholangitis (n=1), cerebellar infarction (n=1), and pulmonary embolism (n=1), but no treatment-related death occurred.
Conclusions
DEB-TACE may be a therapeutic option for advanced HCC patients with PVI.

Review Article
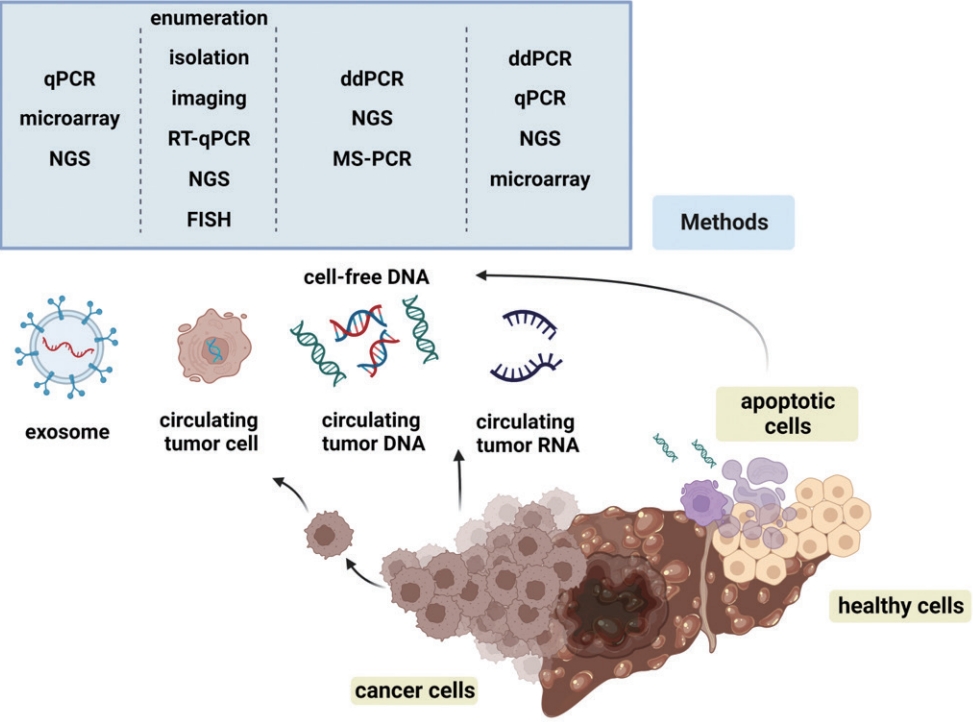
- Liquid biopsy for early detection and therapeutic monitoring of hepatocellular carcinoma
- Eun-Ji Choi, Young-Joon Kim
- J Liver Cancer. 2022;22(2):103-114. Published online September 22, 2022
- DOI: https://doi.org/10.17998/jlc.2022.09.08
- 3,560 Views
- 138 Downloads
- 5 Citations
-
Abstract
PDFSupplementary Material
- Advances in our knowledge of the molecular characteristics of hepatocellular carcinoma (HCC) have enabled significant progress in the detection and therapeutic prediction of HCC. As a non-invasive alternative to tissue biopsy, liquid biopsy examines circulating cellular components such as exosomes, nucleic acids, and cell-free DNA found in body fluids (e.g., urine, saliva, ascites, and pleural effusions) and provides information about tumor characteristics. Technical advances in liquid biopsy have led to the increasing adoption of diagnostic and monitoring applications for HCC. This review summarizes the various analytes, ongoing clinical trials, and case studies of United States Food and Drug Administrationapproved in vitro diagnostic applications for liquid biopsy, and provides insight into its implementation in managing HCC.
-
Citations
Citations to this article as recorded by
- Biomarcatori tumorali: tra diagnostica clinica e medicina di precisione
Rossana FRANZIN
La Rivista Italiana della Medicina di Laboratorio.2024;[Epub] CrossRef - 16S rRNA Next-Generation Sequencing May Not Be Useful for Examining Suspected Cases of Spontaneous Bacterial Peritonitis
Chan Jin Yang, Ju Sun Song, Jeong-Ju Yoo, Keun Woo Park, Jina Yun, Sang Gyune Kim, Young Seok Kim
Medicina.2024; 60(2): 289. CrossRef - Current status of ultrasonography in national cancer surveillance program for hepatocellular carcinoma in South Korea: a large-scale multicenter study
Sun Hong Yoo, Soon Sun Kim, Sang Gyune Kim, Jung Hyun Kwon, Han-Ah Lee, Yeon Seok Seo, Young Kul Jung, Hyung Joon Yim, Do Seon Song, Seong Hee Kang, Moon Young Kim, Young-Hwan Ahn, Jieun Han, Young Seok Kim, Young Chang, Soung Won Jeong, Jae Young Jang, J
Journal of Liver Cancer.2023; 23(1): 189. CrossRef - Correspondence on Letter regarding “Long-term prognosis and the need for histologic assessment of chronic hepatitis B in the serological immune tolerant phase”
Jeong-Ju Yoo, Sang Gyune Kim
Clinical and Molecular Hepatology.2023; 29(2): 513. CrossRef - Exploring the Role of Circulating Cell-Free RNA in the Development of Colorectal Cancer
Chau-Ming Kan, Xiao Meng Pei, Martin Ho Yin Yeung, Nana Jin, Simon Siu Man Ng, Hin Fung Tsang, William Chi Shing Cho, Aldrin Kay-Yuen Yim, Allen Chi-Shing Yu, Sze Chuen Cesar Wong
International Journal of Molecular Sciences.2023; 24(13): 11026. CrossRef
- Biomarcatori tumorali: tra diagnostica clinica e medicina di precisione
Case Reports
- Hepatocellular carcinoma with Budd-Chiari syndrome due to membranous obstruction of the inferior vena cava with long-term follow-up: a case report
- Choong Hee Kim, Gwang Hyeon Choi, Hee Young Na, Chang Jin Yoon, Jai Young Cho, Sangmi Jang, Ji Hye Kim, Eun Sun Jang, Jin-Wook Kim, Sook-Hyang Jeong
- J Liver Cancer. 2022;22(2):194-201. Published online September 15, 2022
- DOI: https://doi.org/10.17998/jlc.2022.08.24
- 2,344 Views
- 55 Downloads
-
Abstract
PDF
- Membranous obstruction of the inferior vena cava (MOVC) is a rare subset of Budd-Chiari syndrome (BCS) with a subacute onset that is often complicated by cirrhosis and hepatocellular carcinoma (HCC). Here we report a case of recurrent HCC in a patient with cirrhosis and BCS that was treated with several episodes of transarterial chemoembolization followed by surgical tumorectomy, whereas the MOVC was successfully treated with balloon angioplasty followed by endovascular stenting. The patient was followed up for 9.9 years without anticoagulation and experienced no stent thrombosis. After the tumorectomy, the patient was HCC-free for 4.4 years of follow-up.
- Long-term Survival of a Patient with a Large Hepatocellular Carcinoma with Main Portal Vein Tumor Thrombosis and Spontaneous Tumor Rupture
- Hyung-Woo Lee, Gi-Ae Kim, Chi Hyuk Oh, Jae-Jun Shim, Byung-Ho Kim
- J Liver Cancer. 2020;20(2):148-153. Published online September 30, 2020
- DOI: https://doi.org/10.17998/jlc.20.2.148
- 3,577 Views
- 72 Downloads
-
Abstract
PDF
- Optimal treatments for patients with advanced hepatocellular carcinoma (HCC) are still limited and their prognosis remains dismal. Yet, there have been rare cases that have shed light on longer survival in these patients assisted by various treatments. This paper aims to present an extraordinary case of far advanced HCC that had been properly managed in spite of continuous recurrence. A patient visited the hospital with a ruptured large HCC with main portal vein tumor thrombosis but survived longer than 14 years owing to active and prompt interventions.
- Combined Transarterial Chemoembolization and External Beam Radiotherapy in a Patient with Recurrent Huge Hepatocellular Carcinoma after Hepatic Resection
- Jesang Yu, Jinhong Jung, Sang Min Yoon
- J Liver Cancer. 2020;20(1):90-97. Published online March 31, 2020
- DOI: https://doi.org/10.17998/jlc.20.1.90

- 3,375 Views
- 79 Downloads
-
Abstract
PDF
- The optimal treatment strategy for unresectable huge hepatocellular carcinoma (HCC) is yet to be established. Non-surgical monotherapy demonstrated insufficient oncologic outcomes in previously reported studies. To improve the clinical outcomes of unresectable huge HCC, combined locoregional treatments can be considered in selected cases. Here, we report a case of 58-year-old male patient who was treated with combined transarterial chemoembolization (TACE) and external beam radiotherapy for recurrent HCC after a previous hepatic resection. After combined TACE and radiotherapy for the intrahepatic lesion, two metastases were diagnosed in the pelvic bones and lung; each lesion was successfully treated with salvage radiotherapy. During the long-term follow-up period (around 8 years 7 months after combined TACE and radiotherapy for the recurrent huge HCC), no definite viable tumors were observed in any of the treated liver, bone, and lung lesions.
- Lipiodol Pneumonitis Following Transcatheter Arterial Chemoembolization for Hepatocellular Carcinoma
- Sungkeun Kim, Hee Yeon Kim, Su Lim Lee, Young Mi Ku, Yoo Dong Won, Chang Wook Kim
- J Liver Cancer. 2020;20(1):60-66. Published online March 31, 2020
- DOI: https://doi.org/10.17998/jlc.20.1.60

- 5,109 Views
- 140 Downloads
- 1 Citation
-
Abstract
PDF
- Transcatheter arterial chemoembolization (TACE) is a useful palliative therapeutic modality for hepatocellular carcinoma (HCC). Postembolization syndromes, such as fever, abdominal pain, and elevated liver enzyme levels are commonly known complications of TACE. One post-TACE pulmonary complication, lipiodol pneumonitis, is rarely reported. Lipiodol pneumonitis after TACE appears to be associated with chemical injury due to accidental perfusion of lipiodol to the lung vasculature, promoted by arteriovenous shunts within the hypervascular HCC. Here, we report a 42-year-old man with unresectable HCC and hepatic vein thrombosis. The patient was initially treated with TACE. The following day after TACE, acute respiratory symptoms such as dyspnea and cough developed with decreased oxygen saturation. Chest X-ray and computed tomography showed multiple patches and diffuse ground-glass opacities in both lung fields, suggesting of lipiodol pneumonitis. The patient’s condition and radiologic abnormalities subsequently improved after 2 weeks of conservative treatment alone.
-
Citations
Citations to this article as recorded by- Lipiodol-induced Pneumonitis Following Transcatheter Arterial Chemoembolization for Hepatocellular Carcinoma
Heechul Nam
The Korean Journal of Gastroenterology.2022; 80(5): 233. CrossRef
- Lipiodol-induced Pneumonitis Following Transcatheter Arterial Chemoembolization for Hepatocellular Carcinoma
- Hepatocellular Carcinoma with Segmental Portal Vein Invasion Exhibiting a Complete Response after Transarterial Radioembolization
- Jun Sik Yoon, Su Jong Yu, Yun Bin Lee, Eun Ju Cho, Jeong-Hoon Lee, Yoon Jun Kim, Jung-Hwan Yoon
- J Liver Cancer. 2019;19(2):159-164. Published online September 30, 2019
- DOI: https://doi.org/10.17998/jlc.19.2.159

- 5,324 Views
- 73 Downloads
-
Abstract
PDF
- The treatment options available for patients with hepatocellular carcinoma (HCC) with portal vein invasion (PVI) include sorafenib, transarterial radioembolization (TARE), radiation therapy (RT), transarterial chemoembolization with RT, and proton beam irradiation. Herein, we present a case of HCC with segmental PVI that was managed via TARE. The patient had a 4 cm HCC that invaded the segment VIII portal vein branch without extrahepatic spread. Liver function was Child-Pugh grade A, and performance status was good. TARE was performed without any adverse events, and a radiological complete response (CR) was achieved. Thereafter, the patient was followed-up every 3-6 months without any further treatment, and the CR was maintained for >3 years. Therefore, TARE may be a useful alternative therapeutic option for patients with HCC exhibiting segmental PVI.
- Combination Therapy of Angiotherapy, Radiation Therapy, and Radiofrequency Ablation for Pulmonary Metastasis of Hepatocellular Carcinoma Accompanied by Nontuberculous Mycobacteria
- Sang Hyun Park, Seul Ki Kim, Ji Hye Kim, Seokgyo Seo, Hyun Pyo Hong, Soo-Youn Ham, Byung Ik Kim
- J Liver Cancer. 2019;19(1):79-84. Published online March 31, 2019
- DOI: https://doi.org/10.17998/jlc.19.1.79
- 3,293 Views
- 52 Downloads
-
Abstract
PDF
- With the advances in hepatocellular carcinoma (HCC) treatment, the lung metastasis of HCC is becoming increasingly important. In treating the lung metastasis of HCC, a multidisciplinary approach can lead to better results than systemic chemotherapy alone. Here, we report on a patient who presented with pulmonary masses, while the HCC was being controlled in the abdominal cavity. The presence of nontuberculous mycobacteria was identified during the diagnosis of the pulmonary masses. The pulmonary metastases of HCC were treated with a combination of angiotherapy, radiation therapy, and radiofrequency ablation. The patient showed a satisfactory progress with this multidisciplinary localized treatment. We report the clinical progress and review the recent literature regarding the treatment of pulmonary metastasis without intrahepatic HCC herein.
Review Article
- Conventional Chemoembolization for Hepatocellular Carcinoma: Role of Cone-Beam Computed Tomography Guidance
- In Joon Lee, Jin Wook Chung
- J Liver Cancer. 2019;19(1):19-29. Published online March 31, 2019
- DOI: https://doi.org/10.17998/jlc.19.1.19
- 5,241 Views
- 145 Downloads
- 4 Citations
-
Abstract
PDF
- Conventional chemoembolization using Lipiodol-based regimens was introduced in the 1980s, and it is currently recommended as the primary treatment modality for patients with unresectable, intermediate, or locally advanced hepatocellular carcinoma (HCC) by the international guidelines. For better therapeutic efficacy and safety, chemoembolization should be performed as selectively as possible through tumor-feeding arteries, based on the detection of arterial supply to the HCC. With the technical advancement of flat-panel detector, cone-beam computed tomography (CBCT) is mounted on the C-arm of the angiographic machine. CBCT facilitates the detection of small occult HCCs and fine tumor-feeding arteries, recognition of extrahepatic collateral supply, navigation of a microcatheter to the target feeding arteries, prevention of non-target embolization, and intraprocedural assessment of the completeness of treatment with chemoembolization. These functions performed by CBCT ultimately improve the safety and efficacy of chemoembolization and may contribute to improving the prognosis of the patient with HCC.
-
Citations
Citations to this article as recorded by- Transarterial Chemoembolization for Hepatocellular Carcinoma: 2023 Expert Consensus-Based Practical Recommendations of the Korean Liver Cancer Association
Yuri Cho, Jin Woo Choi, Hoon Kwon, Kun Yung Kim, Byung Chan Lee, Hee Ho Chu, Dong Hyeon Lee, Han Ah Lee, Gyoung Min Kim, Jung Suk Oh, Dongho Hyun, In Joon Lee, Hyunchul Rhim
Korean Journal of Radiology.2023; 24(7): 606. CrossRef - Transarterial chemoembolization for hepatocellular carcinoma: 2023 expert consensus-based practical recommendations of the Korean Liver Cancer Association
Yuri Cho, Jin Woo Choi, Hoon Kwon, Kun Yung Kim, Byung Chan Lee, Hee Ho Chu, Dong Hyeon Lee, Han Ah Lee, Gyoung Min Kim, Jung Suk Oh, Dongho Hyun, In Joon Lee, Hyunchul Rhim
Journal of Liver Cancer.2023; 23(2): 241. CrossRef - Transarterial chemoembolization for hepatocellular carcinoma: 2023 Expert consensus-based practical recommendations of the Korean Liver Cancer Association
Yuri Cho, Jin Woo Choi, Hoon Kwon, Kun Yung Kim, Byung Chan Lee, Hee Ho Chu, Dong Hyeon Lee, Han Ah Lee, Gyoung Min Kim, Jung Suk Oh, Dongho Hyun, In Joon Lee, Hyunchul Rhim
Clinical and Molecular Hepatology.2023; 29(3): 521. CrossRef - The efficacy of TACE; how can automated feeder software help?
Hassan Abdelsalam, Doaa M. Emara, Ehab M. Hassouna
Egyptian Journal of Radiology and Nuclear Medicine.2022;[Epub] CrossRef
- Transarterial Chemoembolization for Hepatocellular Carcinoma: 2023 Expert Consensus-Based Practical Recommendations of the Korean Liver Cancer Association
Original Article
- Transarterial Chemolipiodolization for Hepatocellular Carcinoma with Central Bile Duct Invasion Causing Conjugated Hyperbilirubinemia: Safety and Prognostic Factors for Survival
- Yang, Keungmo , Sung, Pil Soo , Oh, Jung Suk , Chun, Ho Jong , Jang, Jeong Won , Bae, Si Hyun , Choi, Jong Young , Yoon, Seung Kew
- J Liver Cancer. 2018;18(2):121-129. Published online September 30, 2018
- DOI: https://doi.org/10.17998/jlc.18.2.121
- 2,362 Views
- 39 Downloads
- 2 Citations
-
Abstract
PDF
- Background/Aim
s: The treatments and outcomes of hepatocellular carcinoma (HCC) with bile duct invasion are not well known. We aimed to confirm the safety of transarterial chemolipiodolization (TACL) and identify prognostic factors for patients with bile duct invasion treated with TACL.
Methods
Fifty patients with central bile duct invasion treated with TACL between 2005 and 2017 were enrolled. Patients were divided into three groups: hyperbilirubinemia (total bilirubin ≥2.5 mg/dL) with pre-TACL biliary drainage, hyperbilirubinemia without biliary drainage, and without hyperbilirubinemia. Tumor response to TACL, survival outcomes, length of hospitalization, adverse events using Common Terminology Criteria for Adverse Events (CTCAE), and factors affecting overall survival were compared.
Results
TACL-induced changes of mean CTCAE grades for albumin, alanine aminotransferase, creatinine, prothrombin time, and platelet were not significantly different among patients with or without initial hyperbilirubinemia. Serum bilirubin level was not significantly changed after TACL in all the three groups. Overall survival was not significantly different among the three groups (P=0.097). On multivariate analysis, alpha-fetoprotein <400 ng/dL (hazard ratio [HR]=0.477, P=0.048) and highest total bilirubin level of <2.5 mg/dL within one month after TACL (HR=0.335, P=0.004) were significantly associated with longer survival.
Conclusions
TACL was a safe treatment for HCC patients with central bile duct invasion, irrespective of the presence of initial hyperbilirubinemia. -
Citations
Citations to this article as recorded by- Proton Beam Therapy in Managing Unresectable Hepatocellular Carcinoma with Bile Duct Invasion
Ching-Hsin Lee, An-Hsin Chen, Sheng-Ping Hung, Cheng-En Hsieh, Jeng-Hwei Tseng, Po-Jui Chen, Jen-Yu Cheng, Joseph Tung-Chieh Chang, Kun-Ming Chan, Shi-Ming Lin, Chen-Chun Lin, Wei-Ting Chen, Wan-Yu Chen, Bing-Shen Huang
Cancers.2022; 14(7): 1616. CrossRef - An Analysis for Survival Predictors for Patients with Hepatocellular Carcinoma Who Failed to Sorafenib Treatment in Pre-regorafenib Era
Chan Uk Lee, Young-Sun Lee, Ji Hoon Kim, Minjin Lee, Sehwa Kim, Young Kul Jung, Yeon Seok Seo, Hyung Joon Yim, Jong Eun Yeon, Kwan Soo Byun
Journal of Liver Cancer.2019; 19(2): 117. CrossRef
- Proton Beam Therapy in Managing Unresectable Hepatocellular Carcinoma with Bile Duct Invasion
Review Articles
- Treatment and Surveillance of Hepatocellular Carcinoma in Elderly Patients
- Rho, Seoung Yoon , Lee, Hyun Woong , Kim, Kyung Sik
- J Liver Cancer. 2018;18(2):103-114. Published online September 30, 2018
- DOI: https://doi.org/10.17998/jlc.18.2.103
- 2,235 Views
- 69 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) is the third most common cancer in the digestive system based on survey of domestic cancer incidence, and the ratio of elderly aged 65 or older is expected to rise steadily, leading to a higher incidence of total hepatocellular carcinoma. The most important thing in treating these older patients with HCC is to assess the benefits and risks of the treatment in advance. In other words, the benefit of treatment should be greater than the reduction of survival period or maladjustment due to treatment. Based on these perspectives, we examined how the detailed treatment of hepatocellular carcinoma differs from that of general treatment in elderly patients. In conclusion, older age was not a definite prognostic factor of survival risk-benefit comparison in the most treatment modalities. However it should be carefully considered and approached about possible complications in treating HCC in elderly patients.
- Tumor Response Evaluation after Treatment and Post-treatment Surveillance of Hepatocellular Carcinoma
- Yoon, Jun Sik , Park, Soo Young
- J Liver Cancer. 2018;18(1):9-16. Published online March 31, 2018
- DOI: https://doi.org/10.17998/jlc.18.1.9
- 8,659 Views
- 209 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma is one of the most prevalent malignancies and frequent causes of death worldwide. Treatment options of hepatocellular carcinoma consist of locoregional therapy, surgical resection, liver transplantation, and systemic therapy. Assessment of tumor response is required in patients receiving locoregional and systemic therapy. The Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 is widely used tumor response evaluation criteria. However, the RECIST does not reflect the extent of tumor necrosis after some locoregional therapies and molecular targeted agents. The Modified RECIST (mRECIST), which has the concept of viable tumor, was introduced in order to overcome this problem. The mRECIST were developed on the basis of RECIST version 1.1 and only tumoral tissue showing contrast uptake in arterial phase of dynamic radiologic imaging techniques was measured to assess tumor response. Recently, immune checkpoint inhibitors have emerged as a promising therapeutic modality for the treatment of hepatocellular carcinoma. To identify tumor response after immunotherapy, immune RECIST (iRECIST) has been proposed as consensusbased criteria. After achieving complete response after curative treatment, optimal surveillance was needed to detect recurrence. Individualized surveillance schedule should be considered, taking into consideration the risk factors of the patient and the risk associated with the treatment modalities.
Case Reports
- A Case of Advanced Hepatocellular Carcinoma with Long-term Post-progression Survival under Repeated Transarterial Chemoembolization after Sorafenib Failure
- Jihyun Lee, Hwi Young Kim, Yong Jin Jung, Tae Hun Kim, Kwon Yu
- J Liver Cancer. 2017;17(1):82-87. Published online March 31, 2017
- DOI: https://doi.org/10.17998/jlc.17.1.82
- 1,636 Views
- 8 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma is the third leading cause of cancer related mortality worldwide. Only 30% of patients are eligible for curative surgical resection at diagnosis. For patients with advanced hepatocellular carcinoma with accompanying portal vein tumor thrombosis, Sorafenib is recommended as first-line treatment. However, survival gain from sorafenib is unsatisfactory, and there is no standard therapy for patients who are intolerable or refractory to sorafenib. Here we report a case of a 52-year-old man who initially achieved partial response after sorafenib treatment, but eventually showed disease progression and was treated subsequently with transarterial chemoembolization (TACE). Multinodular recurrence occurred, but he was treated with repeated TACE, and has survived for 4 years so far.
- A Case of Early Multiply Recurred Hepatocellular Carcinoma after Surgical Resection in Patient Who Unprecedented Chronic Liver Disease
- Wang Yong Choi, Byoung Kuk Jang, Woo Jin Chung, Jae Seok Hwang
- J Liver Cancer. 2015;15(2):112-117. Published online September 30, 2015
- DOI: https://doi.org/10.17998/jlc.15.2.112
- 873 Views
- 4 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) have relatively well known causative factors such as chronic hepatitis B, chronic hepatitis C, alcoholic liver disease, Non-alcoholic fatty liver disease (NAFLD), liver cirrhosis and so on. Recently, interesting reports that HCC in the absence of cirrhosis or other chronic liver disease and HCC associated with NAFLD and metabolic syndrome are increasing in USA. So far, there is no report about these issues in Korea. We present a 65 yearold obesity male who had no preceding chronic liver disease history. He was diagnosed as primary HCC and the mass was removed completely. However, HCC recurred shortly after operation. Multiple recurred HCC were treated with transcatheter arterial chemoembolization. (J Liver Cancer 2015;15:112-117)
- Spontaneous Regression of Recurred Hepatocellular Carcinoma with Multiple Lung Metastases
- Beom Yong Yoon, Heon Young Lee, Se Woong Hwang, Se Young Park, Hye Jin Kim, Hye Won Jang,, Byung Seok Lee
- J Liver Cancer. 2015;15(1):46-51. Published online March 31, 2015
- DOI: https://doi.org/10.17998/jlc.15.1.46
- 933 Views
- 6 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) is the most common form of liver malignancy. Spontaneous regression of HCC is extremely rare phenomenon and mechanism of regression remains obscure. 75-year-old woman previously diagnosed with hepatitis C virus-related liver cirrhosis was found to have single mass in liver with elevation of α-fetoprotein level to 10,320 ng/mL. Transarterial chemoembolization (TACE) was performed. 27 months after TACE recurred HCC with multiple lung nodules were confirmed. The patient refused any therapeutic modality. The patient underwent follow-up without any anti-cancer treatment. 8 months after recurrence follow up computed tomography scan revealed spontaneous regression of HCC and completely disappeared lung nodules. The patient is currently doing well and without any evidence of recurrence. The causes of spontaneous regression of HCC are not well understood. Proposed mechanisms are ischemic injury, biological factors, herbal medicine, immunological variations. Further studies are necessary to improve our understanding of this rare phenomenon.
 First
First Prev
Prev


 Follow JLC on Twitter
Follow JLC on Twitter