 E-submission
E-submission
Search
- Page Path
- HOME > Search
Review Article
- Current perspectives on radiotherapy in hepatocellular carcinoma management: a comprehensive review
- Dowook Kim, Jun-Sang Kim
- J Liver Cancer. 2024;24(1):33-46. Published online March 25, 2024
- DOI: https://doi.org/10.17998/jlc.2024.02.26
- 362 Views
- 39 Downloads
-
 Abstract
Abstract
 PDF
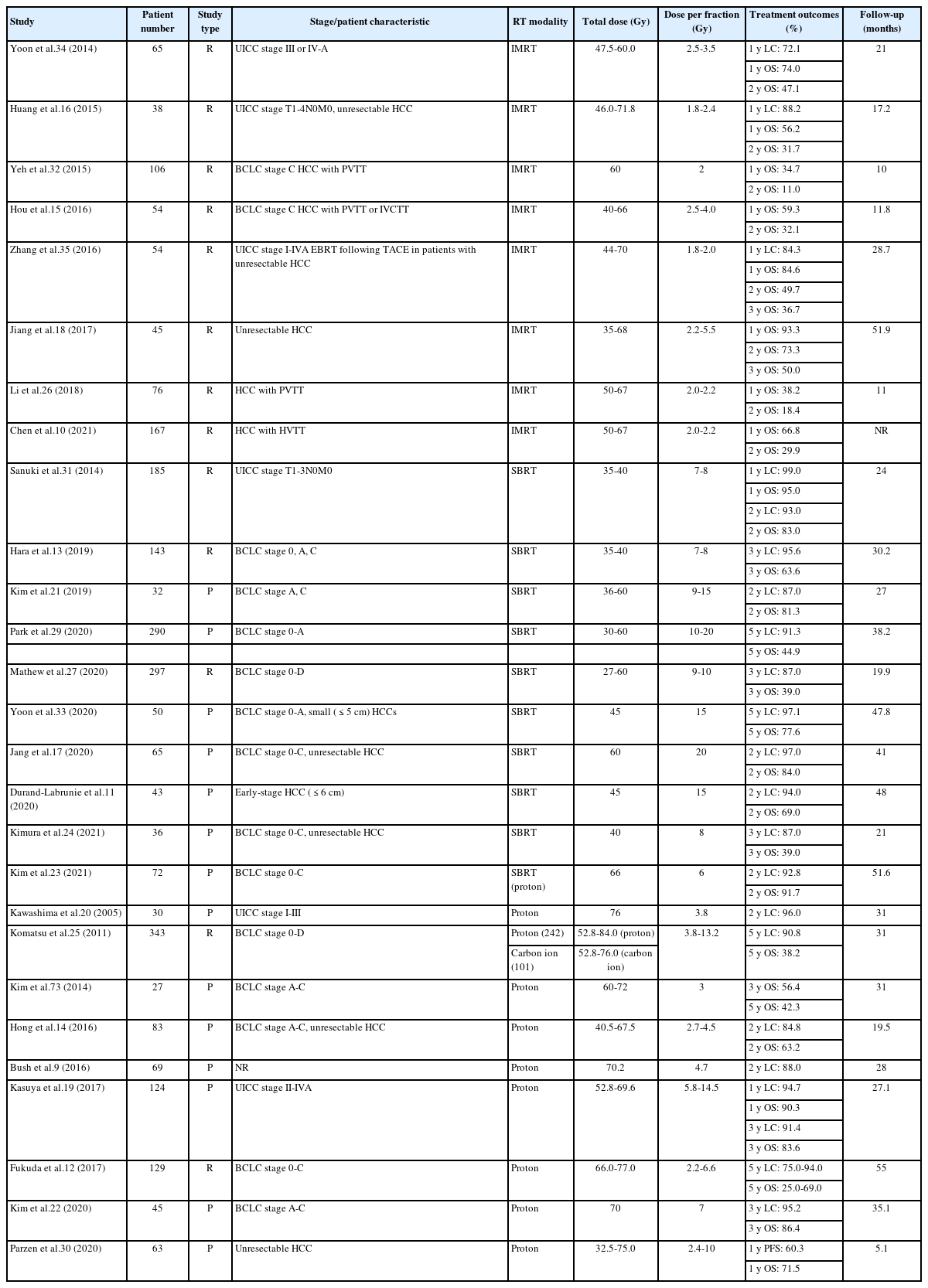
PDF - This review examines the transformative role of external beam radiotherapy (EBRT) in managing hepatocellular carcinoma (HCC), spotlighting the progression from traditional EBRT techniques to advanced modalities like intensity-modulated radiotherapy (RT), stereotactic body RT (SBRT), and innovative particle therapy, including proton beam therapy and carbon ion RT. These advancements have significantly improved the precision and efficacy of RT, marking a paradigm shift in the multimodal management of HCC, particularly in addressing complex cases and enhancing local tumor control. The review underscores the synergistic potential of integrating RT with other treatments like transarterial chemoembolization, systemic therapies such as sorafenib, and emerging immunotherapies, illustrating enhanced survival and disease control outcomes. The efficacy of RT is addressed for challenging conditions, including advanced HCC with macrovascular invasion, and RT modalities, like SBRT, are compared against traditional treatments like radiofrequency ablation for early-stage HCC. Additionally, the review accentuates the encouraging outcomes of particle therapy in enhancing local control and survival rates, minimizing treatment-related toxicity, and advocating for continued research and clinical trials. In conclusion, the integration of RT into multimodal HCC treatment strategies, coupled with the emergence of particle therapy, is crucial for advancing oncologic management, emphasizing the need for relentless innovation and personalized treatment approaches.

Original Articles
- Treatment options for solitary hepatocellular carcinoma ≤5 cm: surgery vs. ablation: a multicenter retrospective study
- Kazuya Kariyama, Kazuhiro Nouso, Atsushi Hiraoka, Hidenori Toyoda, Toshifumi Tada, Kunihiko Tsuji, Toru Ishikawa, Takeshi Hatanaka, Ei Itobayashi, Koichi Takaguchi, Akemi Tsutsui, Atsushi Naganuma, Satoshi Yasuda, Satoru Kakizaki, Akiko Wakuta, Shohei Shiota, Masatoshi Kudo, Takashi Kumada
- J Liver Cancer. 2024;24(1):71-80. Published online November 6, 2023
- DOI: https://doi.org/10.17998/jlc.2023.09.11
- 811 Views
- 92 Downloads
- 3 Citations
-
Abstract
PDF
- Background/Aim
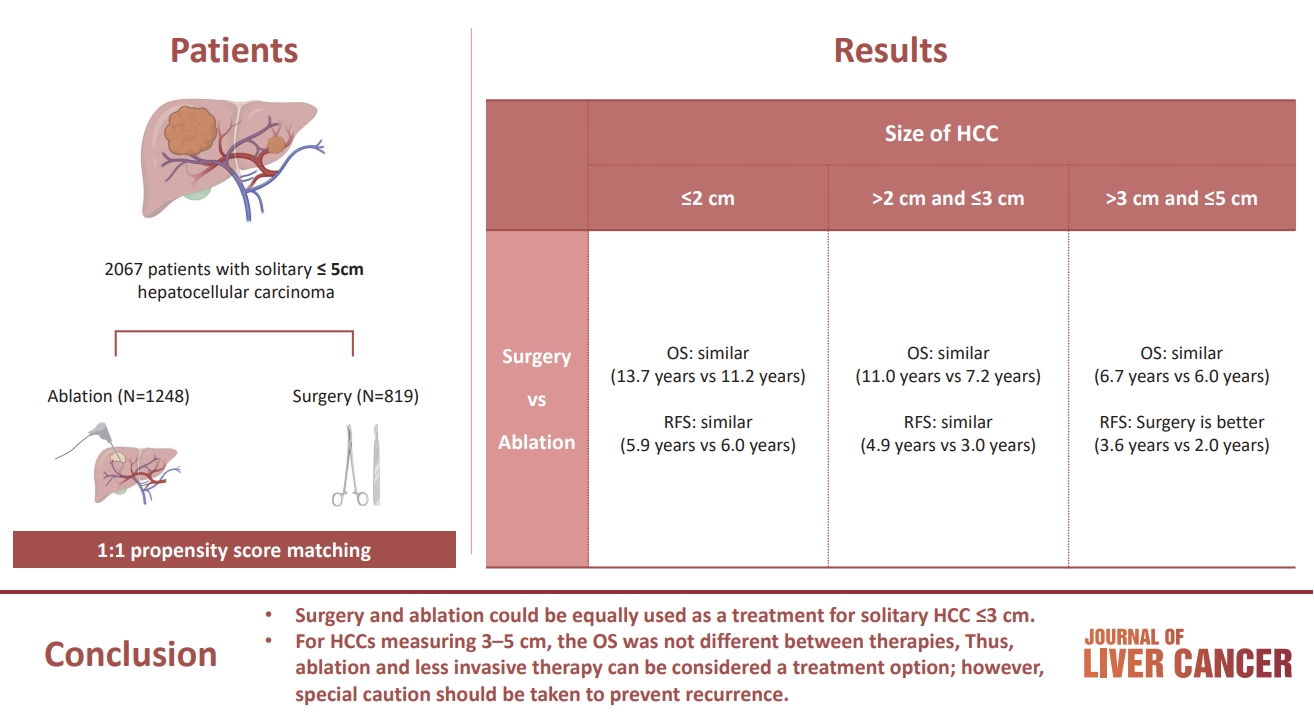
The aim of this study was to compare the therapeutic efficacy of ablation and surgery in solitary hepatocellular carcinoma (HCC) measuring ≤5 cm with a large HCC cohort database.
Methods
The study included consecutive 2,067 patients with solitary HCC who were treated with either ablation (n=1,248) or surgery (n=819). Th e patients were divided into three groups based on the tumor size and compared the outcomes of the two therapies using propensity score matching.
Results
No significant difference in recurrence-free survival (RFS) or overall survival (OS) was found between surgery and ablation groups for tumors measuring ≤2 cm or >2 cm but ≤3 cm. For tumors measuring >3 cm but ≤5 cm, RFS was significantly better with surgery than with ablation (3.6 and 2.0 years, respectively, P=0.0297). However, no significant difference in OS was found between surgery and ablation in this group (6.7 and 6.0 years, respectively, P=0.668).
Conclusion
The study suggests that surgery and ablation can be equally used as a treatment for solitary HCC no more than 3 cm in diameter. For HCCs measuring 3-5 cm, the OS was not different between therapies; thus, ablation and less invasive therapy can be considered a treatment option; however, special caution should be taken to prevent recurrence. -
Citations
Citations to this article as recorded by
- Reply to the Letter regarding “Treatment options for solitary hepatocellular carcinoma ≤5 cm: surgery vs. ablation: a multicenter retrospective study”
Kazuhiro Nouso, Kazuya Kariyama
Journal of Liver Cancer.2024; 24(1): 5. CrossRef - Radiofrequency for hepatocellular carcinoma larger than 3 cm: potential for applications in daily practice
Ji Hoon Kim, Pil Soo Sung
Journal of Liver Cancer.2024; 24(1): 1. CrossRef - Letter regarding “Treatment options for solitary hepatocellular carcinoma ≤5 cm: surgery vs. ablation: a multicenter retrospective study”
Jongman Kim
Journal of Liver Cancer.2024; 24(1): 3. CrossRef
- Reply to the Letter regarding “Treatment options for solitary hepatocellular carcinoma ≤5 cm: surgery vs. ablation: a multicenter retrospective study”
- The efficacy of treatment for hepatocellular carcinoma in elderly patients
- Han Ah Lee, Sangheun Lee, Hae Lim Lee, Jeong Eun Song, Dong Hyeon Lee, Sojung Han, Ju Hyun Shim, Bo Hyun Kim, Jong Young Choi, Hyunchul Rhim, Do Young Kim
- J Liver Cancer. 2023;23(2):362-376. Published online September 14, 2023
- DOI: https://doi.org/10.17998/jlc.2023.08.03
- 1,254 Views
- 70 Downloads
-
Abstract
PDF
 Supplementary Material
Supplementary Material - Background/Aim
Despite the increasing proportion of elderly patients with hepatocellular carcinoma (HCC) over time, treatment efficacy in this population is not well established.
Methods
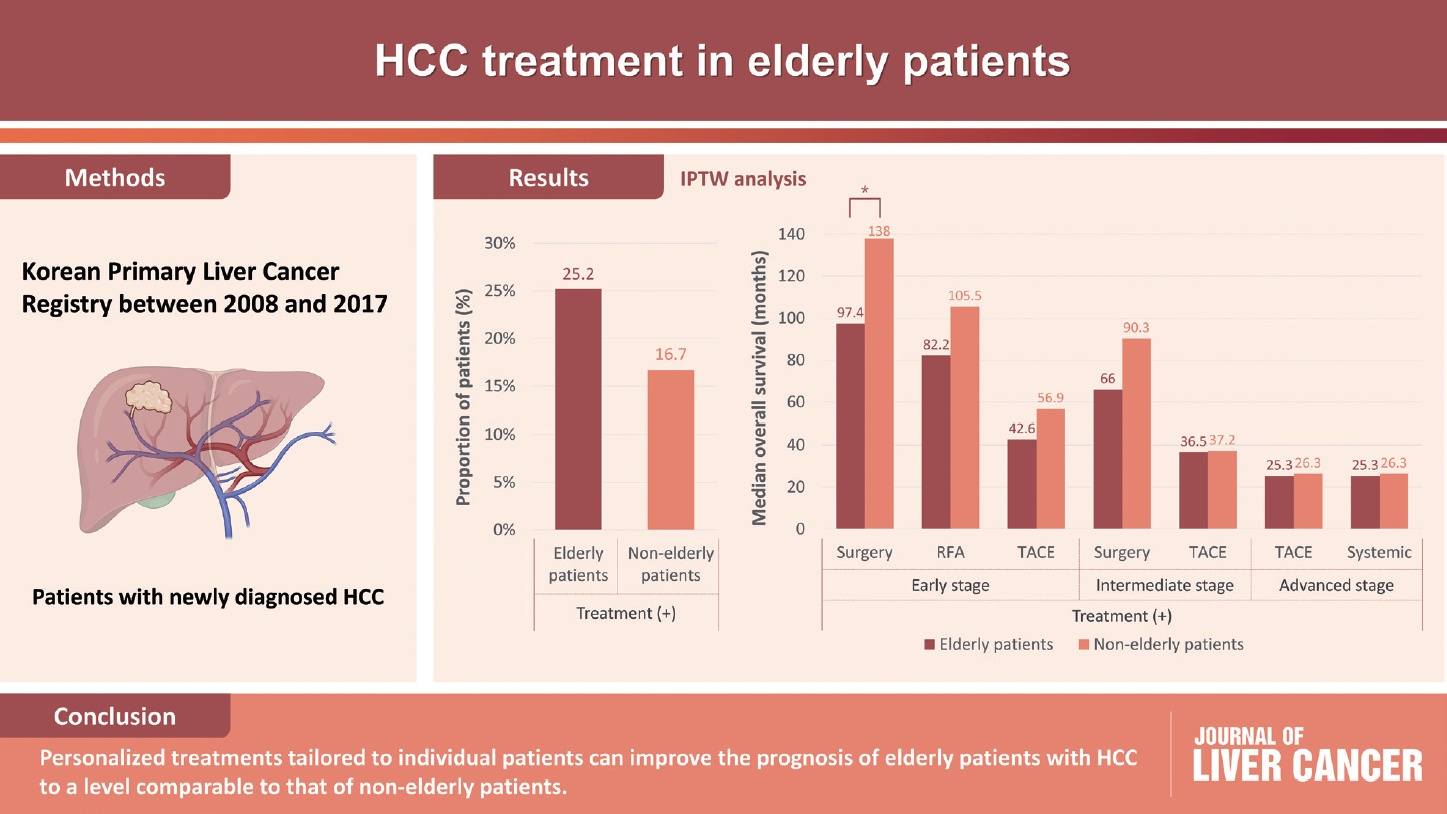
Data collected from the Korean Primary Liver Cancer Registry, a representative cohort of patients newly diagnosed with HCC in Korea between 2008 and 2017, were analyzed. Overall survival (OS) according to tumor stage and treatment modality was compared between elderly and non-elderly patients with HCC.
Results
Among 15,186 study patients, 5,829 (38.4%) were elderly. A larger proportion of elderly patients did not receive any treatment for HCC than non-elderly patients (25.2% vs. 16.7%). However, OS was significantly better in elderly patients who received treatment compared to those who did not (median, 38.6 vs. 22.3 months; P<0.001). In early-stage HCC, surgery yielded significantly lower OS in elderly patients compared to non-elderly patients (median, 97.4 vs. 138.0 months; P<0.001), however, local ablation (median, 82.2 vs. 105.5 months) and transarterial therapy (median, 42.6 vs. 56.9 months) each provided comparable OS between the two groups after inverse probability of treatment weighting (IPTW) analysis (all P>0.05). After IPTW, in intermediate-stage HCC, surgery (median, 66.0 vs. 90.3 months) and transarterial therapy (median, 36.5 vs. 37.2 months), and in advanced-stage HCC, transarterial (median, 25.3 vs. 26.3 months) and systemic therapy (median, 25.3 vs. 26.3 months) yielded comparable OS between the elderly and non-elderly HCC patients (all P>0.05).
Conclusions
Personalized treatments tailored to individual patients can improve the prognosis of elderly patients with HCC to a level comparable to that of non-elderly patients.
- Indications for open hepatectomy in the era of laparoscopic liver resection: a high volume single institutional study
- Sung Jun Jo, Jinsoo Rhu, Jong Man Kim, Gyu-Seong Choi, Jae-Won Joh
- J Liver Cancer. 2022;22(2):146-157. Published online September 14, 2022
- DOI: https://doi.org/10.17998/jlc.2022.08.22
- 2,237 Views
- 60 Downloads
- 2 Citations
-
Abstract
PDFSupplementary Material
- Background/Aim
Since the introduction of laparoscopy for liver resection in the 1990s, the performance of laparoscopic liver resection (LLR) has been steadily increasing. However, there is currently no data on the extent to which laparoscopy is used for liver resection. Herein, we investigated the extent to which laparoscopy is performed in liver resection and sought to determine whether surgeons prefer laparoscopy or laparotomy in the posterosuperior (PS) segment.
Methods
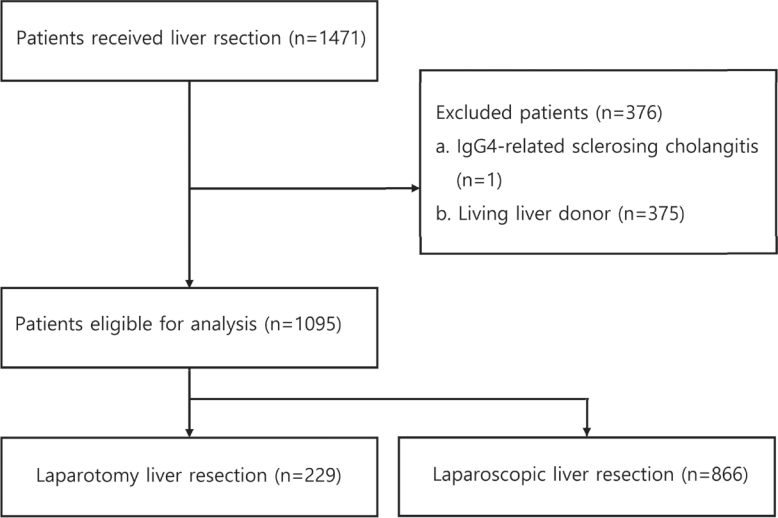
For this retrospective observational study, we enrolled patients who had undergone liver resection at the Samsung Medical Center between January 2020 and December 2021. The proportion of LLR in liver resection was calculated, and the incidence and causes of open conversion were investigated.
Results
A total of 1,095 patients were included in this study. LLR accounted for 79% of the total liver resections. The percentage of previous hepatectomy (16.2% vs. 5.9%, P<0.001) and maximum tumor size (median 4.8 vs. 2.8, P<0.001) were higher in the open liver resection (OLR) group. Subgroup analysis revealed that tumor size (median 6.3 vs. 2.9, P<0.001) and surgical extent (P<0.001) in the OLR group were larger than those in the LLR group. The most common cause of open conversion (OC) was adhesion (57%), and all OC patients had tumors in the PS.
Conclusions
We investigated the recent preference of practical surgeons in liver resection, and found that surgeons preferred OLR to LLR when treating a large tumor located in the PS. -
Citations
Citations to this article as recorded by- Radiofrequency Ablation versus Surgical Resection in Elderly Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis
Jeong-Ju Yoo, Sujin Koo, Gi Hong Choi, Min Woo Lee, Seungeun Ryoo, Jungeun Park, Dong Ah Park
Current Oncology.2024; 31(1): 324. CrossRef - A systematic review and meta-analysis of blood transfusion rates during liver resection by country
Seonju Kim, Yun Kyung Jung, Kyeong Geun Lee, Kyeong Sik Kim, Hanjun Kim, Dongho Choi, Sumi Lee, Boyoung Park
Annals of Surgical Treatment and Research.2023; 105(6): 404. CrossRef
- Radiofrequency Ablation versus Surgical Resection in Elderly Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis
Case Reports
- Fibrolamellar hepatocellular carcinoma that was successfully treated with surgical resection: a case report
- Seong Kyun Na
- J Liver Cancer. 2022;22(2):178-182. Published online June 22, 2022
- DOI: https://doi.org/10.17998/jlc.2022.06.10

- 1,997 Views
- 64 Downloads
- 1 Citation
-
Abstract
PDF
- Fibrolamellar hepatocellular carcinoma (FLHCC) is a rare malignant hepatic cancer with characteristics that differ from those of typical hepatocellular carcinoma (HCC). Unlike conventional HCC, FLHCC is common in young patients without any underlying liver disease and is known to be associated with a unique gene mutation. This cancer type is rare in Asia, with only a few cases being reported in Korea. We report a case of FLHCC in a young woman that successfully underwent surgical resection. The efficacy of alternative treatments, such as transarterial chemoembolization or systemic chemotherapies, has not yet been established. To conclude, early diagnosis and appropriate surgical resection are important for the treatment of FLHCC.
-
Citations
Citations to this article as recorded by- Fibrolamellar Hepatocellular Carcinoma (FLHCC) in a Young Patient Presenting With Nausea and Vomiting After a Greasy Meal
Mohamed Ismail , Sahiba Singh, Menna-Allah Elaskandrany , David s Kim, Yazan Abboud, Michael Bebawy, Abena Oduro, Ritik mahaveer Goyal, Omar Mohamed , Weizheng Wang
Cureus.2024;[Epub] CrossRef
- Fibrolamellar Hepatocellular Carcinoma (FLHCC) in a Young Patient Presenting With Nausea and Vomiting After a Greasy Meal
- Hepatocellular Carcinoma Arising from Hepatocellular Adenoma in an Elderly Male Patient
- Manuel Lim, Jong Man Kim, Ji Eun Kwon, Eun Sung Jeong, Jaehun Yang, Okjoo Lee, Kyeong Deok Kim, Sang Jin Kim, Jinsoo Rhu, Gyu-Seong Choi, Jae-Won Joh
- J Liver Cancer. 2021;21(1):87-91. Published online March 31, 2021
- DOI: https://doi.org/10.17998/jlc.21.1.87

- 3,942 Views
- 95 Downloads
- 1 Citation
-
Abstract
PDF
- Hepatocellular adenoma is a benign tumor of the liver occurring predominantly in young women taking oral contraceptives. The malignant transformation of hepatocellular adenoma into hepatocellular carcinoma has rarely been reported. Herein, we report the case of an elderly male patient with hepatocellular carcinoma that developed from hepatocellular adenoma. The patient’s high risk for surgery and conflicting biopsy and imaging results made it difficult to determine the treatment direction. Eventually, the mass was completely removed by laparoscopic left hemi-hepatectomy without complications.
-
Citations
Citations to this article as recorded by- Radiofrequency Ablation versus Surgical Resection in Elderly Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis
Jeong-Ju Yoo, Sujin Koo, Gi Hong Choi, Min Woo Lee, Seungeun Ryoo, Jungeun Park, Dong Ah Park
Current Oncology.2024; 31(1): 324. CrossRef
- Radiofrequency Ablation versus Surgical Resection in Elderly Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis
Review Article
- Is Transarterial Chemoembolization Only Treatment Option in Patients with Intermediate Stage of Hepatocellular Carcinoma?: in Perspectives of Surgery
- Ji Young Lim, Minjong Lee, Tae Hun Kim
- J Liver Cancer. 2020;20(2):113-119. Published online September 30, 2020
- DOI: https://doi.org/10.17998/jlc.20.2.113
- 3,819 Views
- 130 Downloads
-
Abstract
PDF
- In the Barcelona Clinic Liver Cancer staging system, intermediate stage hepatocellular carcinoma (HCC) is defined as large multinodular tumors without vascular invasion or extrahepatic spread in an asymptomatic patient with good performance status. Intermediate stage HCC includes various subgroups and it is characterized by extensive heterogeneity. Current guidelines recommend transarterial chemoembolization (TACE) as the standard treatment modality for patients with intermediate stage HCC. Although TACE provides improved survival benefits compared with supportive care for patients with intermediate stage HCC, all of them are not good candidates for TACE. TACE refractoriness is another obstacle to effective treatment of patients with intermediate stage HCC. Given that many studies recently reported improved survival in patients treated with hepatic resection over TACE, we reviewed the survival outcomes of TACE and hepatic resection as a treatment strategy of intermediate stage HCC.
Case Reports
- Complete Remission with Transarterial Chemoembolization in a Patient with Hepatocellular Carcinoma Who Showed Early Recurrence following Surgical Resection
- Kim, Hee Yeon , Kim, Chang Wook , Kim, Sungkeun , Lee, Soo Lim , Ku, Young Mi , Won, Yoo Dong
- J Liver Cancer. 2018;18(2):162-167. Published online September 30, 2018
- DOI: https://doi.org/10.17998/jlc.18.2.162
- 1,663 Views
- 25 Downloads
-
Abstract
PDF
- Although surgical resection is a curative treatment option for solitary hepatocellular carcinoma, high recurrence rate contributes to dismal long-term prognosis after curative resection. Early recurrence within 2 years after surgery is associated with intrahepatic metastasis of primary tumor. Liver regeneration after hepatic resection can accelerate tumorigenesis in remnant liver. Treatment strategies for intrahepatic recurrence after curative resection include salvage transplantation, repeated resection, local ablation, and transarterial chemoembolization (TACE). Here, we report a 51-year-old male who was presented with a single large tumor located at segment 4. The patient was initially treated with surgical resection, but intrahepatic recurrence occurred only 4 months after surgery. He achieved complete remission with repeated TACE and has survived without recurrence for 4 years so far.
- A Case of Successful Hepatic Resection after Insufficient Response to Transarterial Chemoembolization and Radiation Therapy in Hepatocellular Carcinoma with Portal Vein Invasion
- Seong Kyun Na, Hyung Joon Yim, Sang Jun Suh, Young Kul Jung
- J Liver Cancer. 2016;16(2):118-122. Published online September 30, 2016
- DOI: https://doi.org/10.17998/jlc.16.2.118
- 915 Views
- 5 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) with portal vein invasion has a poor prognosis. Treatments such as transarterial chemoembolization (TACE), radiation therapy (RT), sorafenib are done as a first line treatment. But in case of incomplete response to first line treatment, there’s no established guideline about salvage treatment. We present a 47 year-old male who was diagnosed as HCC with portal vein invasion. He was treated with RT and repeated TACE, but remnant viable tumor was observed. Surgical resection was performed as a salvage treatment, and HCC was completely removed. He has been followed up over 3 years, but there was no recurrence.
- Long Term Survival in Patient with Hepatocellular Carcinoma after Surgical Resection of Brain Metastasis: A Case Report
- Jeong-Ho Lee, Hyung-Min Yu, Sung-Bum Cho
- J Liver Cancer. 2016;16(1):38-41. Published online March 31, 2016
- DOI: https://doi.org/10.17998/jlc.16.1.38
- 991 Views
- 35 Downloads
-
Abstract
PDF
- Brain metastasis is a rare condition of extraheptaic metastases in hepatocellular carcinoma (HCC). Patients with hepatocellular carcinoma and brain metastasis have rapidly worsened neurologic signs and symptoms, therefore it is regarded to oncologic emergency. Current recommended treatments for brain metastasis are surgical resection or gamma-knife surgery with/without whole brain radiation therapy (RT). However, patients with brain metastasis have a very poor prognosis after adequate treatment. Here, we report a 62-year-old man with HCC and brain metastasis who had long term survival after surgical resection and whole brain RT. (J Liver Cancer 2016;16:38-41)
Review Articles
- Beyond BCLC in the management of patients with HCC 수술적 치료의 적응증
- Dong-Sik Kim
- J Liver Cancer. 2015;15(1):1-3. Published online March 31, 2015
- DOI: https://doi.org/10.17998/jlc.15.1.1
- 862 Views
- 7 Downloads
-
Abstract
PDF
- Although surgical resection can provide best treatment outcome with curative intent, patients with relatively early stage of hepatocellular carcinoma (HCC) can get benefit of this treatment. Barcelona Clinic Liver Cancer (BCLC) staging system limits surgical resection to patients with single HCC with well-preserved liver function, which is often challenged in real practice, especially from Asian countries. During last two decades, surgical outcomes have made remarkable progress approaching zero mortality in many reports. In this review, areas that surgical indications can be expanded beyond BCLC staging system will be discussed, especially in Asian population. (Journal of Liver Cancer 2015;15:1-3)
- Can Radiofrequency Ablation Replace Surgical Treatment of Hepatocellular Carcinoma?
- Min Woo Lee
- Journal of the Korean Liver Cancer Study Group. 2012;12(2):109-112. Published online September 30, 2012
- 568 Views
- 1 Download
-
Abstract
PDF
- According to updated BCLC guideline, radiofrequency ablation (RFA) is now accepted as a standard treatment for hepatocellular carcinomas (HCCs) smaller than 2 cm in diameter in patients who are not considered for liver transplantation. This is because of acceptable local tumor control and survival gain of RFA for small HCCs compared to those of surgical resection. However, for RFA to be a standard treatment of small HCCs, not only expertise of operator but also optimal guiding and ablation techniques such as fusion imaging, contrast-enhanced ultrasonography, artificial ascites, and switching monopolar RFA using multiple electrodes are necessary. Since RFA and surgical resection are equally effective for very early stage HCC; tumor location (i.e., central vs. peripheral location, proximity to central bile duct) and individual condition of patients should be taken into consideration for choosing appropriate treatment. Microwave ablation, which is an emerging thermal ablation technique, is expected to play a key role in the local ablation therapy of small HCCs in the near future. However, more evidence and data is required to verify the efficacy of microwave ablation for the treatment of small HCCs.
Case Reports
- A Case of Advanced Hepatocellular Carcinoma Treated with Curative Surgical Resection after Downstaging by Hepatic Arterial Infusion Chemotherapy
- Jong Ryul Eun, Heon Ju Lee, Jae Woon Kim, Jay Chun Chang, Sung Su Yun, Joon Hyuk Choi
- Journal of the Korean Liver Cancer Study Group. 2011;11(1):60-64. Published online February 28, 2011
- 506 Views
- 2 Downloads
-
Abstract
PDF
- Cure by single modality for advanced hepatocellular carcinoma (HCC) is difficult. Therefore, multidisciplinary approaches are needed to get a better outcome for advanced HCC. In this paper, we report a case of advanced HCC treated with curative surgical resection after downstaging by hepatic arterial infusion chemotherapy (HAIC). A 50-year-old male patient had a maximum 16.0 cm sized HCC in the right lobe. He achieved a partial response after 2 cycles of HAIC with 5-FU (750 mg/m2) and cisplatin (25 mg/m2). After completion of 6 cycles, he received a curative right hepatectomy and the histopathology revealed 95% of tumor necrosis. He is under follow-up without recurrence at 14 months of surgery. This case suggests that surgery after downstaging by HAIC may provide good clinical outcome in advanced HCC.
- A Case of Hepatocellular Carcinoma Who had Surgical Resection Following TACE and Sorafenib Chemotherapy
- Geum Youb Noh, Chul Ju Han, Youn Joo Kim, Ki Young Yang, Su Cheol Park, Jin Kim, Yu Cheol Kim, Yoon Hee Choi, Hyo Rak Lee
- Journal of the Korean Liver Cancer Study Group. 2011;11(1):65-68. Published online February 28, 2011
- 497 Views
- 0 Download
-
Abstract
PDF
- Surgical resection for hepatocellular carcinoma (HCC) is one of the managements, showing improved long term survival. Nowadays, it is being accepted as the main curative treatment. However, the biggest problem we used to face is that surgery cannot be applied at the point of presentation in many patients due to advanced stage. Here we present a case of 54 years old female, who had transarterial chemoembolization (TACE) and sorafenib due to advanced stage of HCC, and later underwent curative surgery due to remarkable response. She had a CT scan of abdomen, which showed multiple huge masses. HCC was confirmed by ultrasonography-guided liver biopsy. TACE was performed once. After TACE, the size of masses increased. Therefore, sorafenib was administered and then continued for 9 months. As partial response was obtained at that time, surgical resection was successfully done. In the pathological report of removed tumor, we could confirm total necrosis of tumor. Now, its been 6 months and she is followed up without any recurrence.
Review Article
- Partial Hepatectomy vs. Radiofrequency Ablation for Treatment of Hepatocellular Carcinoma
- Moon Seok Choi
- Journal of the Korean Liver Cancer Study Group. 2010;10(1):17-21. Published online June 30, 2010
- 518 Views
- 4 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) is the third most common cause of death from cancer in men and the sixth most common cause in women worldwide. Fortunately, significant improvement in prognosis of HCC has been noted from increasing early diagnosis of HCC since the introduction of surveillance and from outstanding progress in various treatment modalities. Radiofrequency ablation (RFA) effectively controls by temperature changes from high-frequency alternating current via electrodes placed within the tissue to achieve coagulation necrosis and tissue desiccation. RFA has been commonly applied as an alternative curative therapy to surgical resection for small HCC due to effective local tumor control. Several previous studies comparing the outcomes of surgery and RFA for HCC have reported variable results probably caused by differences in the study protocol. We compared indication, limitation, therapeutic results of partial hepatectomy and percutaneous RFA to provide better understanding of current status of the two treatment modality and hopefully to give some useful advices for setting up treatment strategy.
 First
First Prev
Prev


 Follow JLC on Twitter
Follow JLC on Twitter